Category Archives: Healthy Living
“A Single Death is a Tragedy, a Million Deaths is a Statistic”
 When I was diagnosed with Stage four metastatic lung cancer, I pledged to launch a series of articles on tobacco, cancer, and related health issues. They won’t be in-depth, but I hope they will be thought-provoking.
When I was diagnosed with Stage four metastatic lung cancer, I pledged to launch a series of articles on tobacco, cancer, and related health issues. They won’t be in-depth, but I hope they will be thought-provoking.
For this first entry, I have turned to history for yet another lesson. The headlined quote about deaths comes from Josef Stalin, the brutal Russian Dictator who became one of the world’s greatest mass murderers, said to be responsible for the deaths of up to 25 million people, a staggering number that overwhelms even Hitler’s brutality.
Chinese leader Mao Zedong was an even more prolific  killer. History records that his “Great Leap Forward” movement, killed 45 million of his own people in just four years. Again, though, the numbers are so great they are meaningless statistics. The human mind can visualize 10, 20, or even 100 bodies, but 45 million dead bodies? Hardly, so the number has little or no visual effect.
killer. History records that his “Great Leap Forward” movement, killed 45 million of his own people in just four years. Again, though, the numbers are so great they are meaningless statistics. The human mind can visualize 10, 20, or even 100 bodies, but 45 million dead bodies? Hardly, so the number has little or no visual effect.
 The deaths caused by Stalin and Mao pale, though, when compared to the numbers piled up by the likes of Pierre Lorillard, Richard Joshua Reynolds, Phillip Morris and others whose tobacco companies are collectively responsible for the deaths of up to a hundred million people in the 20th century. That toll, according to WHO (the World Health Organization) is on track to kill over one billion people in the 21st century.
The deaths caused by Stalin and Mao pale, though, when compared to the numbers piled up by the likes of Pierre Lorillard, Richard Joshua Reynolds, Phillip Morris and others whose tobacco companies are collectively responsible for the deaths of up to a hundred million people in the 20th century. That toll, according to WHO (the World Health Organization) is on track to kill over one billion people in the 21st century.
Unlike Stalin, Hitler, Mao, and others the Tobacco killers  had a murder for money scheme. They persuaded their victims to purchase the poison that killed them. When I smoked, cigarettes were fairly inexpensive. Still, I calculate averaging 35 cents a pack and smoking 3 to 4 packs a day; I paid R. J. Reynolds some $20,000 to kill me. “Winston’s taste good like a cigarette should,” worked on me. Today at $6.00 or more a pack tobacco profits are even higher.
had a murder for money scheme. They persuaded their victims to purchase the poison that killed them. When I smoked, cigarettes were fairly inexpensive. Still, I calculate averaging 35 cents a pack and smoking 3 to 4 packs a day; I paid R. J. Reynolds some $20,000 to kill me. “Winston’s taste good like a cigarette should,” worked on me. Today at $6.00 or more a pack tobacco profits are even higher.
The first few millions of deaths were not aware that the tobacco leaves wrapped in special paper and sold in fancy boxes posed a danger. But, ironically, it made no difference. They bought the soon to be dubbed “cancer sticks in record numbers even when hundreds of health agencies provided proof of their poisonous properties.
Every death was money in the bank.
 A hundred million, dead. A billion dead. Who can even begin to comprehend that number of bodies? No one! And the tobacco companies counted on it. I’m sure I’ll be tossed into the statistical “forgotten” heap, too, but maybe one or two of my blogs and those of my “Statistical” colleagues will survive to indicate that we were human beings, that we had some value and deserved better. We are not statistics. We are not digital data points; we are people who lived, loved, and added value to our communities. You cannot silence us by diminishing our importance. Your ashtray of statistics will continue to be exposed as a murderous cover-up, as our chorus of protests overwhelms your statistical graves.
A hundred million, dead. A billion dead. Who can even begin to comprehend that number of bodies? No one! And the tobacco companies counted on it. I’m sure I’ll be tossed into the statistical “forgotten” heap, too, but maybe one or two of my blogs and those of my “Statistical” colleagues will survive to indicate that we were human beings, that we had some value and deserved better. We are not statistics. We are not digital data points; we are people who lived, loved, and added value to our communities. You cannot silence us by diminishing our importance. Your ashtray of statistics will continue to be exposed as a murderous cover-up, as our chorus of protests overwhelms your statistical graves.
Better, more talented writers than I have tried and failed to get the message across that “tobacco kills.” And while we’ve had some success, people still smoke and “tobacco company profits are soaring. That great big, ugly tobacco leaf still kills a half million Americans every year. That’s more than alcohol, car accidents, AIDS, illegal drugs (Including opioids), murders, and suicides, combined. Yikes!
I am so incensed by the thought of that many Americans dying from tobacco use; I feel compelled to try again to offer an example of the carnage. The Airbus A-380 that can carry 555 or more passengers is the largest airplane in the world. If two of them crashed every day for a year, and human bodies and body parts covered the crash sites, the toll would equal the number killed by tobacco in a year, and the media would be filled with gory pictures of the crash sites. Politicians voices would dominate the airwaves demanding investigations, newspapers would publish lengthy reports, airline executives would be arrested and jailed, and Airbus would cease to exist.
dying from tobacco use; I feel compelled to try again to offer an example of the carnage. The Airbus A-380 that can carry 555 or more passengers is the largest airplane in the world. If two of them crashed every day for a year, and human bodies and body parts covered the crash sites, the toll would equal the number killed by tobacco in a year, and the media would be filled with gory pictures of the crash sites. Politicians voices would dominate the airwaves demanding investigations, newspapers would publish lengthy reports, airline executives would be arrested and jailed, and Airbus would cease to exist.
 Still, an equal number of people die from smoking and there is no outrage, there are no protests or investigations and no one, not a single tobacco executive is behind bars. Why? Why is my death less important because of the way I died? Why am I a statistic and the others are real people whose pictures dominate the front pages of the world? Why is that? It’s because Stalin’s hypothesis is true. I and others like me are cast into that pile of unbelievable, unimaginable statistics because we die quietly without fanfare and gory
Still, an equal number of people die from smoking and there is no outrage, there are no protests or investigations and no one, not a single tobacco executive is behind bars. Why? Why is my death less important because of the way I died? Why am I a statistic and the others are real people whose pictures dominate the front pages of the world? Why is that? It’s because Stalin’s hypothesis is true. I and others like me are cast into that pile of unbelievable, unimaginable statistics because we die quietly without fanfare and gory  pictures. We died not in fiery crashes but rather coughing, and in pain, one at a time rather than in large groups.
pictures. We died not in fiery crashes but rather coughing, and in pain, one at a time rather than in large groups.
Let’s beam us back to today for a moment. Is there anyone in the developed world who is not aware that smoking cigarettes is deadly? Anyone? We obediently hand over $6.00 or more daily for a package of 20 neatly wrapped rolls of tobacco. Each sports a “Filter” on one end to make the product “safer,” filters that are deadlier than the poisons they hide, filters that help block only the biggest tar particles while letting through the smaller bits that can travel deeper into your lungs. “The design of cigarette filters, allows smokers to inhale more smoke and to think that the smoke is safer because it is smoother,” says senior author Dr. Peter D. Shields from The Ohio State University’s Wexner Medical Center in Columbus. “This applies to all cigarettes, not just the ones that used to be called “lights” and “Ultra-lights,” he says. The fact of the matter is cigarettes will kill you regardless of the brand or health claim.
Let’s make the picture even more human. We all remember the delightful TV show “ The Flintstones.” Jean Vander Pyl who acted in the famous cartoon series wa s also a cancer victim. His son, Michael O’Meara had later said:
s also a cancer victim. His son, Michael O’Meara had later said:
“Everybody on the Flintstones smoked, and all of them ended up dying of smoking-related diseases….. That little cute laugh that Berry and Wilma did with their mouths closed? They came up with that because when they normally laughed, being smokers, they coughed.”
And finally, this. You can call it either Irony or poetic  justice but, R.J. Reynolds Senior, the founder of the company that makes Winston, Camels and other tobacco brands, died of pancreatic cancer, which is tied to tobacco use.
justice but, R.J. Reynolds Senior, the founder of the company that makes Winston, Camels and other tobacco brands, died of pancreatic cancer, which is tied to tobacco use.
R.J. Reynolds the second, died of emphysema which is caused by cigarette smoking.
And R.J. Reynolds the third also died of emphysema.
Sometimes what goes around, really does come around.
Stay tuned.
A former journalist, Governor’s Press Secretary, and  Communications Consultant, Bob Aronson smoked for 37 years. He quit the habit nearly 30 years ago after developing COPD (Chronic Obstructive Pulmonary Disease). A failing heart, probably caused by smoking, resulted in his receiving a heart transplant in 2007. In June of 2018, he was diagnosed with Stage Four Metastatic Lung Cancer, likely caused by his smoking combined with a compromised immune system due to his need for anti-rejection drugs to protect his transplanted heart. He is currently being treated at the Mayo Clinic in Jacksonville, Florida where he lives with his wife Robin and their dogs Reilly and Ziggy.
Communications Consultant, Bob Aronson smoked for 37 years. He quit the habit nearly 30 years ago after developing COPD (Chronic Obstructive Pulmonary Disease). A failing heart, probably caused by smoking, resulted in his receiving a heart transplant in 2007. In June of 2018, he was diagnosed with Stage Four Metastatic Lung Cancer, likely caused by his smoking combined with a compromised immune system due to his need for anti-rejection drugs to protect his transplanted heart. He is currently being treated at the Mayo Clinic in Jacksonville, Florida where he lives with his wife Robin and their dogs Reilly and Ziggy.
Bob’s Newheart. This site contains nearly 300 Blogs on Organ Donation/Transplantation and Related Issues
Feel free to share any of the blogs you find here without permission but with attribution. Your comments are welcome.
The Opioid Epidemic They Don’t Want You To Think About
 Recently on Facebook I posted some thoughts on the opioid crisis. It got a lot of reaction. The opioid crisis of which I speak is not the one that’s in the news every day. This one rarely gets any news coverage.
Recently on Facebook I posted some thoughts on the opioid crisis. It got a lot of reaction. The opioid crisis of which I speak is not the one that’s in the news every day. This one rarely gets any news coverage.
The one with which you are familiar includes criminals, the addiction and death of our children and greedy physicians who dole out narcotics like Halloween candy.
And then … there’s the other one, it involves the thousands if not millions of victims of chronic pain who cannot get relief. That second crisis is just as tragic as the first and is generated to a great degree by fear, distrust, ignorance and a total lack of compassion. Every day there are many, many thousands of Americans who suffer unbearable pain and cannot get relief even though it is available. The politicians and instigators who are responsible for this tragedy are so blinded by their obsession with law and order issues they cannot see the pain and suffering they create in order to satisfy their desire to toss someone in the slammer.
These overly protective know-it-all, know-nothings see a rash of raids where so- called “pill mills” are shut down and physicians and others are rounded up as an epidemic about to sweep away the foundations of our society. In a wild, irrational state of panic they spread ignorance and lies that would have everyone believe that millions are getting painkillers they don’t need from crooked physicians and then selling them on the streets or overdosing.
called “pill mills” are shut down and physicians and others are rounded up as an epidemic about to sweep away the foundations of our society. In a wild, irrational state of panic they spread ignorance and lies that would have everyone believe that millions are getting painkillers they don’t need from crooked physicians and then selling them on the streets or overdosing.
I am not denying there is a problem. I am complaining that it is being approached in a manner that takes no prisoners and treats everyone with suspicion and disrespect. When an ill-conceived policy is enforced with tactics of intimidation and outright threats, then the policymakers become suspect.
If you read the testimony before congress and in other hearings along with news reports it is easy to see how the unbalanced approach to the opioid epidemic is also causing harm. The doomsayers are warning us all that our children will soon become addicts and likely will die because of the irresponsible physicians who write opioid prescriptions for anyone who asks. Their solution? Paint everyone with the same brush. Make it more difficult to get a pain killer prescription than a seat next to the winning coach at the Chapionship game of the final four.
 That’s not to say there isn’t some truth to their crisis claims, but to attempt to shut down narcotics prescriptions all over America is an overreaction that is already generating horrific consequences. This reaction is not dissimilar to the often heard claim that most welfare recipients are cheats and therefore we have to cut welfare programs to the core and beyond.
That’s not to say there isn’t some truth to their crisis claims, but to attempt to shut down narcotics prescriptions all over America is an overreaction that is already generating horrific consequences. This reaction is not dissimilar to the often heard claim that most welfare recipients are cheats and therefore we have to cut welfare programs to the core and beyond.
 What is ignored in this crackdown on opioids is that there are thousands and thousands of people who suffer with chronic pain. I’m one of them, my brother is another and I know many more as well. This overreaction to a problem is causing suffering beyond belief. If you’ve never experienced the kind of pain that has you on your knees, crying and begging for relief, then you have no business judging those who are in that situation. If you’ve never had or seen pain so bad, you pray for a quick death then you have no right to suggest policy. If everything you know about drug abuse comes from talk shows and the internet, you have no right to attempt to interfere in the lives of those who live with it every day.
What is ignored in this crackdown on opioids is that there are thousands and thousands of people who suffer with chronic pain. I’m one of them, my brother is another and I know many more as well. This overreaction to a problem is causing suffering beyond belief. If you’ve never experienced the kind of pain that has you on your knees, crying and begging for relief, then you have no business judging those who are in that situation. If you’ve never had or seen pain so bad, you pray for a quick death then you have no right to suggest policy. If everything you know about drug abuse comes from talk shows and the internet, you have no right to attempt to interfere in the lives of those who live with it every day.
This nationwide irrationality has caused the politicians to pressure the U.S. Drug Enforcement Administration (DEA) and the Food and Drug Administration (FDA) to threaten physicians with overwhelming amounts of paperwork, loss of license and even jail time if they are found to violate or even misinterpret a rule or law. The result is that many physicians just plain refuse to write narcotics prescriptions. There are major healthcare organizations that have adopted the same policy. Most cruel, though, is the action taken by many reputable pain clinics to offer narcotic-free pain relief. Nice claim, but Impossible. No I’m not a doctor but I have intense pain and I know what provides relief and what doesn’t.
result is that many physicians just plain refuse to write narcotics prescriptions. There are major healthcare organizations that have adopted the same policy. Most cruel, though, is the action taken by many reputable pain clinics to offer narcotic-free pain relief. Nice claim, but Impossible. No I’m not a doctor but I have intense pain and I know what provides relief and what doesn’t.
Physicians are so afraid of losing their licenses they are refusing to do what they are trained to do — alleviate suffering. They are also in violation of the “First, do no harm,” mandate. It is time that the AMA and other physician’s organizations along with individuals raise their voices in loud and continuing objection to this insanity. Yes, we need rules, yes we need consumer protection laws but no, we don’t need politicians forcing broad rulings and passing overly broad laws that result in increased suffering, like the kind I described.
I have tried every technique for killing pain known to medical science. None of them worked. Only drugs like Oxycontin, Dilaudid and others give me relief and sometimes they aren’t totally effective. No one is more sensitive to the dangers of narcotics than those who are recovering from dependency on them. Often that dependency is not the patient’s fault but it’s all that’s available to help them. I am a recovering alcoholic. Addiction medicine suggests that if you are addicted to one drug like alcohol, then you are subject to becoming addicted to painkillers as well. I know that to be true and I usually take less of my drug than is prescribed. Fortunately I found a real pain clinic, with board certified pain specialists who have been willing to treat me. I pray from month to month, they will be allowed to continue to practice.
All I’m asking is that common sense and compassion play some part in the national discussion on the prescribing of narcotics and in the enforcement of the laws that govern those who write the prescriptions. When you are stricken with cancer, osteoarthritis (my ailment) and so many other conditions that cause unbearable pain you deserve to be able to get some relief. Doctors deserve to be able to practice medicine. Sure they should be arrested if they break the law, but for the government to flood them with paperwork, warnings and other sorts of intimidating tactics is unforgivable.
 We don’t live in a black and white world. There are many shades of gray. This paranoia about narcotics is the same as the ignorance that suggests that anyone who takes narcotics will be addicted, or any physician who prescribes them is a greedy criminal. It is the same as believing all welfare recipients are cheating the system and immigrants are inherently dangerous. This incredibly narrow minded approach to any problem is the result of a nation that no longer honors education, refuses to read, gets its information from talk shows and rarely thinks beyond the latest talk show or political one-liner. We have become a nation that believes in junk science, junk history, junk education, junk leaders and junk wisdom. You might be happy with that simple approach to life until you find yourself in need of food, heaalthcare, or compassion. I hope that real wisdom strikes our nation before any of the true-believers in that black and white world develop a condition that causes them unbearable physical pain for which no one will provide relief.
We don’t live in a black and white world. There are many shades of gray. This paranoia about narcotics is the same as the ignorance that suggests that anyone who takes narcotics will be addicted, or any physician who prescribes them is a greedy criminal. It is the same as believing all welfare recipients are cheating the system and immigrants are inherently dangerous. This incredibly narrow minded approach to any problem is the result of a nation that no longer honors education, refuses to read, gets its information from talk shows and rarely thinks beyond the latest talk show or political one-liner. We have become a nation that believes in junk science, junk history, junk education, junk leaders and junk wisdom. You might be happy with that simple approach to life until you find yourself in need of food, heaalthcare, or compassion. I hope that real wisdom strikes our nation before any of the true-believers in that black and white world develop a condition that causes them unbearable physical pain for which no one will provide relief.
When we expect to gain knowledge in the same way a dispenser pops out Pez candy we diminish our history, our potential and everything for which our founders stood. A mood of selfishness and unreasonable approaches to law and order has grown deep roots in America. Only when we have restored our moral and ethical compass will we stand a chance of emerging as the thought and compassion leader we like to believe we are.
we diminish our history, our potential and everything for which our founders stood. A mood of selfishness and unreasonable approaches to law and order has grown deep roots in America. Only when we have restored our moral and ethical compass will we stand a chance of emerging as the thought and compassion leader we like to believe we are.
-0-
If you found this blog to be helpful, please share it. Permission is not needed but attribution is appreciaated.
Bob’s Newheart. This site contains nearly 300 Blogs on Organ Donation/Transplantation and Related Issues
Feel free to share any of the blogs you find here without permission but with attribution. Your comments are welcome.
Donor Mom Meets Man with Son’s Heart
When I stand before God at the end of my life, I hope I have given away my talents, my love and my organs and can say, “God I used everything you gave me to benefit others. Anonymous
By Bob Aronson
 The time had come. Claire Connelly was finally going to meet the man who had her son Paul’s heart. She would travel from southern to northern California by train to meet him. This trip was more than just an opportunity to meet the man, it was the culmination of a three-year long search. Claire was determined to let nothi
The time had come. Claire Connelly was finally going to meet the man who had her son Paul’s heart. She would travel from southern to northern California by train to meet him. This trip was more than just an opportunity to meet the man, it was the culmination of a three-year long search. Claire was determined to let nothi ng get in the way of this meeting. She was so afraid that she might oversleep and miss her train, she drove to the Amtrak station the evening before and slept in her van in the parking lot. Meeting her son’s’ heart recipient had become Claire’s sole purpose in life, so when she boarded that train last Monday morning her heart was in her throat.
ng get in the way of this meeting. She was so afraid that she might oversleep and miss her train, she drove to the Amtrak station the evening before and slept in her van in the parking lot. Meeting her son’s’ heart recipient had become Claire’s sole purpose in life, so when she boarded that train last Monday morning her heart was in her throat.
The recipient’s name is Ken, he cherishes his privacy and we agreed to identify him only by that name. He is retired and lives with his wife in a northern California city. Claire was not only invited to meet Ken and his wife, but also to stay in their home for a few days so they could get to know each other
Before we go any further, let me take a moment to remind you who Claire Connelly is.  I wrote about her in a blog on October 21, 2016. To meet her, even by phone is to love her. She is kind, upbeat, considerate and passionate about life and living. Claire is your favorite aunt — you know, the one who is funny, always has a gift for you and really listens to what you have to say. She’s one of those people who brings energy and love of life into any conversation. When you talk; with Claire you can’t help but feel good.
I wrote about her in a blog on October 21, 2016. To meet her, even by phone is to love her. She is kind, upbeat, considerate and passionate about life and living. Claire is your favorite aunt — you know, the one who is funny, always has a gift for you and really listens to what you have to say. She’s one of those people who brings energy and love of life into any conversation. When you talk; with Claire you can’t help but feel good.

Claire’s son Paul
Claire has suffered unimaginable pain in her life. She had three children, two boys and a girl. Now, only the daughter remains. Her son Pete died of cancer at the age of 46 in 2008, and 49-year-old Paul’s life was taken by a stroke in 2013. Losing two sons within five years is tragic enough, but Claire’s pain was compounded because they died on the same date — October 13. “What are the odds,” she asks. “What are the odds that you would lose two sons within five years of one another and on  the same date on the calendar?”
the same date on the calendar?”
When she was called to the hospital in 2013 Paul was on life support. His driver’s license indicated that he was an organ donor, so when asked if she wanted to donate his organs, Claire Agreed immediately. She does not know who got his other organs, but she’s satisfied to know that Ken got his heart.
I could feebly try to describe her feelings about meeting Ken, but that would be wrong. Her own words provide drama and emotion that I could not begin to write. When she got on the train on December 12, she carried with her some gifts for her son’s heart recipient along with a stethoscope so she could listen to his heart. As soon as she boarded, she sent me a text, “On the train. On way to meet Ken,” she said. Her writing describes the stream  of random thoughts that somehow merged like two sets of railroad tracks. Claire kept a journal as the train sped north. If you close your eyes you can almost hear the clacking of the wheels on the track and the whistle being blown as intersections are crossed.
of random thoughts that somehow merged like two sets of railroad tracks. Claire kept a journal as the train sped north. If you close your eyes you can almost hear the clacking of the wheels on the track and the whistle being blown as intersections are crossed.
The words that follow are Claire’s from her journal. When you read them you will have the rare privilege of being able to listen in on a mom’s thoughts as she anticipates hearing her son’s beating heart for the first time in three years.
“Getting to meet Ken is the very best Christmas present I could have ever received, but let me make one thing very clear, this is not my story or Ken’s. My son Paul is the hero here. Long ago he made the decision to become an organ donor. All I did was to ensure that his wishes were fulfilled.
make one thing very clear, this is not my story or Ken’s. My son Paul is the hero here. Long ago he made the decision to become an organ donor. All I did was to ensure that his wishes were fulfilled.
Ken and I have been speaking by phone since August 12 and now I’m actually on the train going to meet him and his wife. He is alive today because my wonderful son Paul made the

Claire and Ken’s wife Janice
courageous decision to become an organ donor.
Ken has expressed his gratitude many times, but more than that he lives his gratitude. This kind gentleman will not drink alcohol or coffee because he has “too much respect” for Paul’s heart! Oh lord, my soul can finally rest knowing that Paul’s heart has found the best possible safe harbor. To know that I gave birth to the heart that is beating within this man’s chest and that he is sharing my own DNA as he sits across from me or goes about his day is something I can barely get my head around!
Recently I found a photo of a Paul when he was just four years old. He was holding his

Jan trimming the tree
fishing pole, Oh how he loved fishing and wouldn’t you know it, Ken loves fishing, too! I had that picture framed to give to Ken because that sport is his passion and I wanted him to know he had the heart of a fisherman. Strange but there were some other links I discovered, too. For example, they both drove the same model of pickup truck and both smoked the same type of Cigarillos.
Because of our telephone, text and email contact, I now have a bond with this remarkable man that is as close as any other I have and it warms my heart to know that he is in this world. What might appear to some as a quick four-day trip would be to miss the point. I’ve been on this journey for three long years, a journey that would reunite me with the essence of Paul. The anticipation of leaving the melancholy life i have known for the past three years and approaching a new fulfilling relationship with my new “son” kept me on the verge of tears until our initial embrace.”
When the train arrived and squeaked and squealed to a slow stop. Claire got up from her seat and headed for the door. Ken and Jan were there waiting for her. The meeting was almost wordless, yet spoke reams. Again, Claire’s words.
“Immediately when I got off the train there were lots of long hugs. It seems as though none of us wanted to let go, but eventually, we got in the car, had a lovely dinner and talked and hugged again till late in the evening.

There were plenty of hugs for everyone
The following day, we spent in our jammies, just hanging out at the house, everyone comfortable with each other. That’s when I brought out the mementos. A coffee mug that said, “I had a change of heart,” Paul’s fishing picture, Paul’s key ring, a special pencil that was engraved with Paul’s name and some other things that I either made or purchased. Ken loved all of them, he even has a collection of keys.
Still in our jammies, we continued to talk as we set up and decorated the Christmas tree. We
had so much fun doing it, it was so meaningful we committed to making it a tradition and doing it every year.
Finally, I hollered into the living room, “Ken, bring that heart in here, I want to listen to it.” I had my stethoscope in my hand.
He stood in front of me and with the earpieces in, I touched the chest piece to where I thought his heart was but heard nothing. I kept trying but couldn’t seem to find it and
It was then that Ken took my hand and the stethoscope chest piece and placed it on his heart. Then — then I heard the soft, steady, rhythm, “Thump thump – thump

After three years she hears Paul’s heart again. A part of her son is still alive.
I was listening to my son’s heart again. My eyes filled with tears and I got a lump in my throat, I couldn’t stop listening. Paul’s heart was keeping this lovely man alive. I thought to myself, I can now rest. The long wait is over and I no longer have to wonder. I am at long last at peace with the world. I finally heard Paul’s heart. A part of my son was alive and well.
Ken told me that just before the transplant, the Surgeon asked him if he wanted to see the heart. When he looked, it started to beat and the doctor said, “This heart wants to live,” and the procedure was started. Ken said he was told that his transplant only took seven hours, a much shorter time than usual. He was also told it was the smoothest, least complicated transplant the Doctor had done.”
Hearts are amazing organs. A man’s heart, for example, beats 70 times a minute. A woman’s heart is a little faster. The thumping sound you hear is really the sound of the four valves opening and closing in a process that pumps a million barrels of blood in an average lifetime. To do so it will beat 2.5 billion times. To put it in perspective, If you were to turn on your kitchen faucet all the way and let it run for 45 years, that would be equivalent to the amount of blood a heart pumps in a lifetime. That’s pretty amazing.
All good things must end it is said, and so it was for this visit. After four days together Ken and Jan took Claire to the train station for the ride home. It was bittersweet. Bitter because she didn’t’ really want to leave, but sweet because she had so many wonderful memories to carry with her and sustain her. Claire finally had some kind of closure. Again, her words.
“When we got to the train, Ken boarded with me to make sure I was comfortable. He seemed very concerned about me and did everything he could to make sure I would have a pleasant trip back home. I sat there for a few minutes and then felt I just had to see him one more time, so I got up and went to the door and, and there he was, waving and saying, “Bye mom, bye.”
Now I’m home again with so many wonderful memories and with so many pictures to remind me of my journey and of my new son. I will go back, we will meet again. I don’t know where or when, but it will happen.”
When Claire spoke of meeting Ken and Jan again, I could almost hear that wonderful song playing in the background.
We’ll meet again
Don’t know where
Don’t know when
But I know
We’ll meet again
Some sunny day
Keep smilin’ through
Just like you
Always do
‘Til the blue skies drive
The dark clouds
Far away
-0-
 Bob Aronson is a 2007 heart transplant recipient and the founder of this blog which contains nearly 300 posts on donation/transplantation and associated issues. If you need a support group, please join Facebook’s Organ Transplant Initiative. And if you are not yet an organ donor, sign up now, it takes almost none of your time and you can do it from where you are sitting. Log on to http://www.donatelife.net and make the commitment now. Then, tell your family your decision so there is no confusion when the time comes.
Bob Aronson is a 2007 heart transplant recipient and the founder of this blog which contains nearly 300 posts on donation/transplantation and associated issues. If you need a support group, please join Facebook’s Organ Transplant Initiative. And if you are not yet an organ donor, sign up now, it takes almost none of your time and you can do it from where you are sitting. Log on to http://www.donatelife.net and make the commitment now. Then, tell your family your decision so there is no confusion when the time comes.
32 Years Of Altruistic Organ Donation and The Death Toll Is Rising. Is it Time For a Change?
By Bob Aronson
 Over the years I’ve written a great deal about organ donation and whether we should continue with the altruistic program we have now, or consider some sort of compensation for organ donors and/or families.
Over the years I’ve written a great deal about organ donation and whether we should continue with the altruistic program we have now, or consider some sort of compensation for organ donors and/or families.
The problem is huge, bigger than huge because 22 people die every day that could have lived had enough people become organ donors.
So, let’s start with the problem. Well, it’s a big one. 120,000 plus people on the waiting list and under 30,000 transplants performed each year with those organs coming from just 13,000 donors. That means you have about a 25% chance of getting a transplant if you can even make it onto the list. That percentage goes down each year because the number of donors is not keeping up with the number of people being added to the list. So, the longer you wait, the less likely you are to get an organ. If you really study those numbers you can understand why patients awaiting new organs are nervous and you can understand the urgency. You see, they are on the list because modern medicine has run out options. These patients have been told they will die unless they get new organs. I was on that list, I know of what I speak. In my case all the stars lined up just right and I got a new heart. I was beyond lucky.
So – from where do the organs come? The answer is that the number of transplantable organs depends entirely on a national voluntary or “altruistic” system where people donate organs out of the goodness of their hearts. We’ve been doing that since NOTA (the National Organ Transplant Act) was passed by congress in 1984. Here is the most current list of human organs that can be transplanted. In case you are wondering, here’s what can be transplanted; liver, kidney, pancreas, kidney/pancreas (can be done at same time), heart, lung, heart/lung (can be done at same time). Intestine, vascularized composite allografts (VCAs), such as face and hand transplantation.
Here’s where I start getting into trouble. Logic would indicate that if a system put in place over 30 years ago keeps falling farther and farther behind the demand, then I cannot help but think the system is failing. The system is not a total failure because it does save many lives, but it is failing because the gap between supply and demand is widening. Now I suspect that some people will argue the “Failing” point, but you can’t argue with the numbers. The system isn’t working. And every time new approaches are proposed, like some sort of compensation, the ethicists loudly proclaim that the practice would be unethical. Ok, but what’s ethical about allowing 8,000 people to die each year because there are not enough organs? Why isn’t someone questioning the ethics of that fact?
over 30 years ago keeps falling farther and farther behind the demand, then I cannot help but think the system is failing. The system is not a total failure because it does save many lives, but it is failing because the gap between supply and demand is widening. Now I suspect that some people will argue the “Failing” point, but you can’t argue with the numbers. The system isn’t working. And every time new approaches are proposed, like some sort of compensation, the ethicists loudly proclaim that the practice would be unethical. Ok, but what’s ethical about allowing 8,000 people to die each year because there are not enough organs? Why isn’t someone questioning the ethics of that fact?
 Before we get into what can be done about the organ shortage we should discuss briefly the two kinds of organ donors. There are living donors, people who can donate one of their two kidneys or a part of a liver. And – there are deceased donors. In both cases insurance will pay for the removal and transplantation of the organs, it costs the donor absolutely nothing. But there are other expenses that are not paid.
Before we get into what can be done about the organ shortage we should discuss briefly the two kinds of organ donors. There are living donors, people who can donate one of their two kidneys or a part of a liver. And – there are deceased donors. In both cases insurance will pay for the removal and transplantation of the organs, it costs the donor absolutely nothing. But there are other expenses that are not paid.
Let’s start with living donors. In order to qualify they must undergo a series of tests, then travel to the transplant site, have a short hospital stay following the recovery of the organ and then travel back home. And, God forbid, there could be complications down the road.
None of those expenses are covered by insurance. When you have to take time off of work to be tested, pay for travel, lodging more time off for the surgery and then travel home again, and maybe suffer complications later, the dollars can begin to add up. Again, logic says there just might be more living donors if their costs were covered. As it is they act as disincentives.
The same, unfortunately, is true for deceased donors and their families. Many of these donors have been hospitalized for a long time before they died. Then, of course, there was terrible grief followed by funeral arrangements. Again, while insurance paid for the recovery of the organs and all medical costs associated with procedure, some families were left with only a, “Thank you,” and a pile of medical bills topped by funeral expenses. Sometimes these burdens are unbearable for families.
 Here’s an example. In 1993 a man later identified as William Michael Lucas, 34, an unemployed man was badly beaten outside his home. He was taken to the hospital and treated, but finally after an extended and expensive hospital stay, succumbed to his massive injuries. It was determined that some of his organs were transplantable and his heart and liver went to Pennsylvania Governor Robert Casey.
Here’s an example. In 1993 a man later identified as William Michael Lucas, 34, an unemployed man was badly beaten outside his home. He was taken to the hospital and treated, but finally after an extended and expensive hospital stay, succumbed to his massive injuries. It was determined that some of his organs were transplantable and his heart and liver went to Pennsylvania Governor Robert Casey.
The transplant was successful and Governor Casey went on to live for another seven years. Not only did Lucas save Governor Casey’s life, everyone who took part in the organ recovery and transplant was paid which includes, clinics, hospitals, surgeons, medical staff, and the Organ Procurement Organization (OPO) among others.
While all this was happening the Lucas family didn’t get a penny. All they got was inconsolable grief and a deluge of medical bills and threats from creditors. It is now well over 20 years since the transplant and a $6,200 funeral still remains unpaid. Somehow, to me, this just isn’t right. Everyone got paid for the role they played in Mr. Lucas’ gift of life — everyone, that is, expect for the Lucas family. Now ask yourself, is that fair?
 I want to be perfectly clear here, I have no problem with those mentioned getting paid, they are all people and organizations with very special skills and they deserve to be compensated. But didn’t the Lucas family deserve some consideration. Wouldn’t it make just a little bit of sense to relieve them of the medical bills and the funeral burden and maybe some grief counseling, too? That seems only fair.
I want to be perfectly clear here, I have no problem with those mentioned getting paid, they are all people and organizations with very special skills and they deserve to be compensated. But didn’t the Lucas family deserve some consideration. Wouldn’t it make just a little bit of sense to relieve them of the medical bills and the funeral burden and maybe some grief counseling, too? That seems only fair.
I am not suggesting for a moment that families get paid, that there be a cash value for organs. That would be wrong and it would violate U.S. law. It is illegal to sell or buy human organs. I have to believe, though, that people might give organ donation a little more consideration if they knew that the financial burden that usually goes with it would be relieved.
What I am suggesting is not a radical argument. If Medicare and other insurance coverage can come up with the dollars to pay the huge costs of paying transplant teams and all the others associated with the procedure, they certainly can find a way to defray the costs to the donor.
Medicare could easily find the money to do this if they were allowed to do two things. One ![]() is to negotiate the price of prescription drugs and the other is to pay for anti-rejection drugs beyond the three year limit which is in effect now for non-Medicare enrolled patients.
is to negotiate the price of prescription drugs and the other is to pay for anti-rejection drugs beyond the three year limit which is in effect now for non-Medicare enrolled patients.
As a part of the Medicare Part D. Agreement under President George W. Bush insurance companies were talked into cooperating by guaranteeing them they could charge Medicare whatever their retail price was for drugs. In other words, Medicare was not allowed to negotiate the price of drugs. The VA can do that, but not Medicare. Negotiating drug prices would bring them down far enough to pay for the organ donation expenses suffered by some organ donors.
The second issue that would help is this one and it is a doozer. It is so absurd it is beyond one’s ability to comprehend. Of the 120,000 people on the transplant list some 82 percent are Kidney patients. Under a law passed years ago Kidney patients and only Kidney patients who are not of Medicare age can have organ transplants paid for by Medicare and Medicare will pay for anti-rejection drugs for 36 months. If you are of Medicare age the agency will pay for those drugs for the life of the patient.
 This policy makes absolutely no sense because, ironically, Medicare will pay for a lifetime of dialysis if you go into rejection because you can’t afford to buy the drugs that prevent it, Medicare will even pay for another transplant and/or dialysis at costs that are many times the annual expense of immunosuppressant drugs. This political sleight of hand act not only wastes U.S. taxpayer dollars, it can actually cause death.
This policy makes absolutely no sense because, ironically, Medicare will pay for a lifetime of dialysis if you go into rejection because you can’t afford to buy the drugs that prevent it, Medicare will even pay for another transplant and/or dialysis at costs that are many times the annual expense of immunosuppressant drugs. This political sleight of hand act not only wastes U.S. taxpayer dollars, it can actually cause death.
Medicare spends around $90.000 per year for an individual who is on dialysis and $125,000 during the first year of a kidney transplant. However, after that first year the transplant patient’s drug costs plummet to $25,000 or a little over $2,000 a month. Not many people have an easy time paying that bill but for the federal government it would be a cost saving measure to cover the drugs rather than pay for a new transplant or more dialysis. Furthermore, extending immunosuppressive coverage beyond the 36-month post-transplant limit would improve outcomes and enable more kidney patients who lack adequate insurance to consider transplantation. Most transplant recipients also have a higher quality of life, and are more likely to return to work than dialysis patients and if they return to work, they start paying taxes again.
So what are the options for increasing the number of human organs for transplant. Well, the list is not a long one.
Presumed consent. That means everyone is automatically considered a donor unless they opt out and everyone would have that opportunity. Spain is one of the nation’s that has adopted this policy and it has become the world’s leader in organ donation, despite the fact that it still gives families of the prospective donor the right to approve or disapprove of the idea. Spain’s deceased organ donation rate is 36 per one million inhabitants. It is ten less in the United States at 26 per million.
Mandatory organ donation. While this is certainly an option. It is most unlikely. Polls have indicated public opinion is overwhelmingly opposed to such an idea.
The Life Sharers option. Life Sharers is a 12000 member group that pledges to donate organs with the idea that only organ donors should get organs if they should need a transplant. It might be a decent idea, but it has never really caught on and is not growing fast enough to have any significant impact on the organ shortage.
Legalize the sale of human organs. It is unlikely that such a proposal would be approved  in the United States. The only nation in the world that allows for it is Iran and Iran, as a result, has no organ shortage. In Iran Two charities facilitate the process by finding potential vendors and introducing them to the recipients, and are charged with checking the compatibility of a possible donation and ensuring a fair trade. After the transplant, the vendor is compensated by both the government and the recipient. Iranians are not allowed to donate kidneys to non-citizens. In the U.S. the argument against paying people for their organs (living donors of kidneys and livers) is that the practice would prey on the poor. Supposedly only people who are in desperate need of money would sell their organs. “The rich or reasonably well off,” the argument goes, “Don’t need the money so few of them would become donors under such a system.” Additionally, wealthy people could buy organs from the poor but the poor could not afford to buy organs if they needed them.
in the United States. The only nation in the world that allows for it is Iran and Iran, as a result, has no organ shortage. In Iran Two charities facilitate the process by finding potential vendors and introducing them to the recipients, and are charged with checking the compatibility of a possible donation and ensuring a fair trade. After the transplant, the vendor is compensated by both the government and the recipient. Iranians are not allowed to donate kidneys to non-citizens. In the U.S. the argument against paying people for their organs (living donors of kidneys and livers) is that the practice would prey on the poor. Supposedly only people who are in desperate need of money would sell their organs. “The rich or reasonably well off,” the argument goes, “Don’t need the money so few of them would become donors under such a system.” Additionally, wealthy people could buy organs from the poor but the poor could not afford to buy organs if they needed them.
An added emphasis on biomechanical or other organ options like Therapeutic cloning. Chances are pretty good that by the time humans quit bickering about paying for organs in one way or another we will already have organs produced by a combination of science and technology. Certainly a major government commitment should be made in this area.
Limited compensation for organ donors. There is already a precedent of sorts. Human hair and blood has been for sale for decades and covering expenses has some influential supporters.
 Dr. Sally Satel is a Kidney transplant recipient and a resident scholar at the American Enterprise Institute in Washington D.C. She is editor of “When Altruism Isn’t Enough: The Case for Compensating Kidney Donors” (AEI Press, 2009) and a practicing psychiatrist and lecturer at the Yale University School of Medicine. She has long supported the idea of compensating organ donors. You can read the Wall Street Journal story here.
Dr. Sally Satel is a Kidney transplant recipient and a resident scholar at the American Enterprise Institute in Washington D.C. She is editor of “When Altruism Isn’t Enough: The Case for Compensating Kidney Donors” (AEI Press, 2009) and a practicing psychiatrist and lecturer at the Yale University School of Medicine. She has long supported the idea of compensating organ donors. You can read the Wall Street Journal story here.
http://www.wsj.com/articles/SB10001424052748704322004574477840120222788
Dr. Satel has long been a proponent of compensating organ donors. In a publication of the Elder Law Journal, Satel had this to say about compensation for donated organs.
“What kinds of compensation should be offered? A reasonable case could be made for an outright payment. After all, it is hard to argue that an individual is competent enough to sell an organ yet unfit to manage the money he receives in exchange for it.
Donor protection is the linchpin of any compensation model. Standard guidelines for physical and psychological screening, donor education, and informed consent could be formulated by a medical organization, such as the American Society of Transplant Surgeons, or by another entity designated by the federal Department of Health and Human Services. A waiting period of three to six months could be built in to ensure the prospective donor has ample time to think it through. Monitoring post-transplant donor health is important as well.
 One idea is to provide lifetime health insurance, through Medicare or a private insurer for the donor. The donor would receive annual physicals, routine medical screening, and long-term follow-up, in addition to standard health coverage. A federally sponsored registry of donors could help physicians study long-term outcomes for donors and take steps to remedy physical or psychological difficulties that arise.
One idea is to provide lifetime health insurance, through Medicare or a private insurer for the donor. The donor would receive annual physicals, routine medical screening, and long-term follow-up, in addition to standard health coverage. A federally sponsored registry of donors could help physicians study long-term outcomes for donors and take steps to remedy physical or psychological difficulties that arise.
MULTIPLE COMPENSATORS In this scheme, an intermediary broker would coordinate donors, compensators (the entities that pay for the transplants), and medical centers. Medicare would be one of several possible compensators, along with private insurers, charitable foundations, and perhaps a fund established through a surcharge added to the cost paid by insurers and foundations.
PRIVATE CONTRACTS The easiest way to start a market for organs is simply to change the law so as to allow someone who needs an organ and someone who wants to sell one to make their own arrangements through contract—as infertile couples currently do with surrogate mothers. But such a system would inevitably attract criticism because it appears to favor the rich over poor. You can learn more on this subject by checking out these links:
http://www.sallysatelmd.com/html/2007-04-16_ElderLawJournal.pdf http://www.cnn.com/2012/07/03/health/allowed-sell-organs-time/index.htmlhttp://www.npr.org/2008/05/21/90632108/should-we-legalize-the-market-for-human-organshttp://www.newint.org/argument/2010/10/01/human-organ-trade-debate/http://plato.stanford.edu/entries/organs-sale/
“Is it ethical to compensate people for their organs?” Dr. Satel thinks so and offers some interesting options.
“My colleagues and I suggest a system in which compensation is provided by a third party (government, a charity or insurance) with public oversight. Because bidding and private buying would not be permitted, available organs would be distributed to the next in line–not just to the wealthy. Donors would be carefully screened for physical and psychological problems, as is currently done for all volunteer living kidney donors. Moreover, they would be guaranteed follow-up care for any complications.
.Many people are uneasy about offering lump-sum cash payments. A solution is to provide in-kind rewards–such as a down payment on a house, a contribution to a retirement fund, or lifetime health insurance–so the program would not be attractive to people who might otherwise rush to donate on the promise of a large sum of instant cash. The only way to stop illicit markets is to create legal ones. Indeed, there is no better justification for testing legal modes of exchange than the very depredations of the underground market.”
.Dr. Satel and several colleagues have called on congress to reform the 1984 National Organ Transplant Act (NOTA), which makes it a felony to provide material reward for an organ.
 The issue of paying for human organs is controversial to say the least but that does not mean it can’t or won’t work. Iran, which is usually not a good example for much of anything, allows for such a program and the result reportedly is that their waiting list has sharply declined and in some cases it has diminished entirely.
The issue of paying for human organs is controversial to say the least but that does not mean it can’t or won’t work. Iran, which is usually not a good example for much of anything, allows for such a program and the result reportedly is that their waiting list has sharply declined and in some cases it has diminished entirely.
http://freakonomics.blogs.nytimes.com/2008/04/29/human-organs-for-sale-legally-in-which-country/
What we need in the United States is an open dialogue free of emotional outbursts that would allow for a small pilot program to one or more of these ideas. More importantly I am appalled by the attitude in official circles that suggests, “There’s nothing more we can do about increasing the supply of organs.” That’s giving up and I refuse to surrender to such backward thinking. If we can get agreement on sending people to Mars by 2035 we sure could get agreement on putting an end to organ transplant waiting lists. It’s also time for everyone to admit the altruistic approach is simply inadequate. People are dying, 22 of them every day and we are satisfied with that? I think not. There is nothing wrong with admitting failure.
All of the volunteers and others who have worked so hard to increase altruistic organ donation deserve a lot of credit, they’ve saved thousands of lives, but I think they, too, would agree it’s time to stop the dying, it’s time to end the shortage. It’s over 30 years since the altruistic approach was started, how much more time do officials need to admit failure and try other approaches?
The time to act is now. We have a new President and a new congress. It’s time to get them involved in saving lives. That is after all, why they were elected.
-0-
Bob Aronson is a 2007 heart transplant recipient . He is the founder of two social media sites. 1) Facebook’s 4,300 member Organ Transplant Initiative a support group that also offers a wide variety of educational information and 2) this site, Bob’s Newheart. Here you will find nearly 300 blogs on issues surrounding organ donation/transplantation. Your comments are always welcome.
If you are not an organ donor, becoming one is simple. Just go to http://www.donatelife.net and sign up. It only takes a couple of minutes. When you are done tell your family so there’s no confusion when the time comes. That’s all there is to it.
Major Depressive Disorder (MDD) Common Among Transplant Recipients
By Bob Aronson

I have written before about post-transplant depression. It is real, it is common and it can be dangerous, but there is help, lots of it. You do not have to live feeling as though you are a drain on society a waste of skin and a burden to your friends and family. Most importantly you should know that there’s no shame in having a mental illness. It is as real as heart disease or cancer or a broken leg, but it is also treatable. You don’t have to live a life of gloom and doom.
According to Very Well Thttps://www.verywell.com/coping-after-an-organ-transplant-3157200 “There are issues that are unique to organ transplantation that the average surgery patient does not experience. In the majority of cases, a patient who is waiting for an organ knows that for an organ to become available an appropriate donor must die.
There is an emotional struggle between maintaining hope for a transplant and dread, knowing that a stranger will die before that becomes possible. Transplant recipients often acknowledge that they feel survivor’s guilt, having benefited from the death of another.
It is important for recipients to remember that family members of donors report feeling that being able to donate organs was the only positive thing to happen during a heartbreaking time. The correspondence they receive from organ recipients can help the feeling of total loss after a loved one dies.”
As a transplant recipient myself I know the depression I felt prior to the transplant was related to the fear of not getting an organ and dying. A depression hangover from pre to post transplant seems to make sense. You got a new organ, not a new brain and while the reasons may be different, the feeling remains. The most common concern is that “Someone had to die, so that I could live.” But logic dictates that your donor died because it was his or her time to die. Your survival is not even remotely tied to that death. A better more positive thought might be, “I am alive because my donor made the decision to donate while still living. It was a gift to someone who needed an organ and I turned out to be that someone.” Sometimes, though, it is hard to accept and depression becomes a reality.
This blog is aimed at giving you basic information on what depression is, how to deal with it and where to go for more information. I suffer from it, I understand it and I know it is treatable. I’m hoping the following information is helpful.
Major Depressive Disorder is a common disease whether transplant patient or not. Anyone can suffer from it and the suffering can be severe. Let’s start with a little check list to see if you suffer from MDD and need to see a physician to become whole again. If some or all of the following situations apply to you, it is likely you need some help.
- Changes in sleep. Many people have trouble falling asleep, staying asleep or sleeping much longer than they used to. Waking up early in the morning is common for people with major depression.
- Changes in appetite. Depression can lead to serious weight loss or gain when a person stops eating or uses food as a coping mechanism.
- Lack of concentration. A person may be unable to focus during severe depression. Even reading the newspaper or following the plot of a TV show can be difficult. It becomes harder to make decisions, big or small.
- Loss of energy. People with depression may feel profound fatigue, think slowly or be unable to perform normal daily routines.
- Lack of interest. People may lose interest in their usual activities or lose the capacity to experience pleasure. A person may have no desire to eat or have sex.
- Low self esteem. During periods of depression, people dwell on losses or failures and feel excessive guilt and helplessness. Thoughts like “I am a loser” or “the world is a terrible place” or “I don’t want to be alive” can take over.
- Depression can make a person feel that nothing good will ever happen. Suicidal thoughts often follow these kinds of negative thoughts—and need to be taken seriously.
- Changes in movement. People with depression may look physically depleted or they may be agitated. For example, a person may wake early in the morning and pace the floor for hours.
- Physical aches and pains. Instead of talking about their emotions or sadness, some people may complain about a headache or an upset stomach.- See more at: http://www.nami.org/Learn-More/Mental-Health-Conditions/Depression#sthash.X9zhh5bP.dpuf
If you suffer from MDD (Major Depressive Disorder) you should know the following.

human brain
We often hear that depression is caused by a chemical imbalance in the brain. Well, the fact is there is little or no scientific evidence to prove that point. It is a theory that is probably partially true but is really an oversimplification of a very complex disease. The “Chemical Imbalance” description is the result of the pharmaceutical industry’s attempt to make their “Re-balancing” chemicals more popular and desirable.
There are scores of medications that claim to help depression and while some work for at least a short while no one knows for sure how or why they work or how long they might be effective. Attempts at balancing the so-called chemical imbalances are sometimes effective, but not always. That may be because the exact degree of involvement by Serotonin or other chemicals in the cause and treatment of depression is a theory, not a fact. It is far easier to sell a remedy caused by chemical imbalances than one that has multiple causes and interactions.
MDD is a form of mental illness that often requires a multidisciplinary approach. Sometimes pills or capsules will work absent any other form of treatment. Often, though, it may need the broader approach that can only be offered by a Psychiatric clinic. Start with your primary care doc, but if your condition gets more serious seek specialized professional help.
If you suffer from depression as millions of Americans do, it is likely that your doctor has prescribed an anti-depression medication for you like Remeron, Wellbutrin or Cymbalta. Chances are good, too, that if you‘ve been taking anti-depressants for a while you’ve found that after a while they seem to wear out so your doctor will prescribe a new one. There are scores of such medications out there so physicians have a huge variety from which to choose making it is easy to prescribe something different.
doctor has prescribed an anti-depression medication for you like Remeron, Wellbutrin or Cymbalta. Chances are good, too, that if you‘ve been taking anti-depressants for a while you’ve found that after a while they seem to wear out so your doctor will prescribe a new one. There are scores of such medications out there so physicians have a huge variety from which to choose making it is easy to prescribe something different.
Depression is a form of mental illness and for some that’s a shameful problem. They feel they should be able to overcome depression without help. “Depression? Really? You? You’ve got a great job, family, friends, a new car…wow, what’s to be depressed about? You’ve got so much to live for,” is probably one of the most insensitive responses one can give to hearing of someone’s depression, yet it is offered thousands of times a day. It is as though it is somehow illegal or immoral to have a mental illness, but when you feel sad, worthless, lose interest in daily living and even have suicidal thoughts, you need help.
Major Depressive Disorder (MDD) is not only common it is getting worse. Estimates suggest that about 16 million Americans are victims. MDD is a psychiatric disorder that goes well beyond feeling sad or “down.” It can become so severe as to cause you to become disabled or even to want to take your own life. Part of the problem in identifying and treating MDD is that it lives in that shadowy world of mental illness that still carries with it a certain stigma or shame.
Anyone who has suffered from MDD knows how debilitating the disease can be. It isn’t just feeling “Blue” or out of sorts — it is feeling totally useless and without purpose or value. It is feeling as though you are a waste of human organs and skin, have no right to exist and represent a drain on society. It is beyond feeling that you are inferior, it is knowing that you are and therefore knowing there is no hope. It is knowing you are a burden to others and that there is no hope – that’s how bad it is.

A senior couple talking with a marriage counselor. Could also be a salesman in their home.
While talk therapy has always been available, the pharmaceutical companies saw the need for a quicker fix like a pill that could somehow miraculously change your mood. They did a lot of very expensive research and came up with several medication approaches and several of them work very well. Nearly all of them based on the theory that depression was at least in part caused by chemical imbalances in the brain. The pharmaceutical company scientists determined that Serotonin was one of the major chemicals affecting depression and it therefore became the one most often targeted.
The first group of anti-depressants included brand names like Prozac, Paxil and Zoloft. They come from a group of medications called SSRIs (Selective Serotonin Reuptake Inhibitors) and are generally safe and effective. The important fact here is that most if not all anti-depressants are aimed at regulating brain chemicals and there are lots of them. I counted 82 different brand names in an ever so brief internet check on the number of anti-depressants on the market.
The problem is that these drugs don’t always work right away or at all for that matter and it can take time to figure that out. Anti-depressants can also get expensive, Pfizer’s Pristiq, for example can cost over $100 a month with insurance – far more without. On the other hand Duloxetine or Cymbalta can be cheap. I just paid around $10.00 for thirty 30 milligram capsules. Many of these drugs have generics that sell for a lower price so be sure to ask. One thing you can count on is that if you begin to use anti-depressant drugs you will, over time, use several different kinds.
There seems to be three approaches to dealing with MDD. Obviously there is medication and finding the right one could take some time. There’s also Cognitive Behavioral Therapy (talk therapy) and Electroconvulsive Therapy (ECT). Yes, ECT is sending electrical shocks into the brain, but it is not like the Shock Therapy of the old Boris Karloff movies or more recently, “One flew over the Cuckoos nest.” It is brief, painless, has few side effects and can be very effective. To the best of our knowledge most MDD therapies are covered by Medicare and other insurances, but check before you agree to be treated. It is not unusual for some patients to participate in all three forms of treatment.
(ECT). Yes, ECT is sending electrical shocks into the brain, but it is not like the Shock Therapy of the old Boris Karloff movies or more recently, “One flew over the Cuckoos nest.” It is brief, painless, has few side effects and can be very effective. To the best of our knowledge most MDD therapies are covered by Medicare and other insurances, but check before you agree to be treated. It is not unusual for some patients to participate in all three forms of treatment.
For more information on depression we recommend the following links.
Selecting the right anti-depressant http://www.mayoclinic.org/diseases-conditions/depression/in-depth/antidepressants/art-20046273
Cognitive behavioral Therapy http://www.nami.org/Learn-More/Treatment/Psychotherapy
Electroconvulsive Therapy http://www.nimh.nih.gov/health/topics/brain-stimulation-therapies/brain-stimulation-therapies.shtml
Bob Aronson of Bob’s Newheart is a 2007 heart transplant recipient, the founder of Facebook’s over 4,200 member Organ Transplant Initiative (OTI) and the author of most of the nearly 300 posts on this site. You may comment in the space provided or email your thoughts to me at bob@baronson.org. And – please spread the word about the immediate need for more organ donors. There is nothing you can do that is of greater importance. If you convince one person to be an organ and tissue donor you may save or positively affect over 60 lives. Some of those lives may be people you know and love. You can register to be a donor at http://www.donatelife.net. It only takes a few minutes. Then, when registered, tell your family about your decision so there is no confusion when the time comes.
Bob’s Newheart Blogs
This site offers news, information and opinions about organ donation, transplantation and related subjects.
There are nearly 300 posts here covering a wide range of health topics. You may share without permission, but attribution is appreciated.
Thoughtful Communication Can Greatly Enhance Your Quality of life and — It’s Free!
***Note from Bob Aronson. Dr. Priscilla Diffie-Couch is a cousin who understands the power of words. She has contributed several blogs to Bob’s Newheart about a variety of subjects, but all revolve around mental and physical health issues.
Living in the 21st century with all of its stresses like the high cost of healthcare, raising a family and trying to make ends meet has resulted in higher stress levels for many. That stress wears on us and negatively affects our quality of life. Dr. Diffie-Couch says it doesn’t have to be that way. She offers a partial solution — communication. If you do it thoughtfully you likely will feel a whole lot better and the best part of it all is that it is free. You have nothing to lose by trying what she suggests — and you may have a whole lot to gain.
By Dr. Priscilla Diffie-Couch
 Human communication and health are two topics I have been passionate about most of my life. So much so that I got three degrees in one and have spent most of my adult life digging deep into the other. Both are topics of such depth and expanse that no human being could come close to mastering the limitless scope of either. One facet that has especially fascinated me is the effect one has on the other, particularly, the impact that communication has on human health.
Human communication and health are two topics I have been passionate about most of my life. So much so that I got three degrees in one and have spent most of my adult life digging deep into the other. Both are topics of such depth and expanse that no human being could come close to mastering the limitless scope of either. One facet that has especially fascinated me is the effect one has on the other, particularly, the impact that communication has on human health.
You can’t study the science and art of communication without being exposed to the needs and motives that drive human behavior. So you’ll find a bit of that as well as my own personal philosophy of life as you read here what flows from mind to page.
Research now tells us that human beings who are most social live the longest. Once you look into how that happens, you discover that, like everything else of value in life, it is not the quantity but quality of that interaction that has the most pronounced effect on human relationships and thereby on human health.
What it takes too many of us too long to learn in life is that a satisfying  relationship can never be something one party feels and the other does not. It can be judged only in the eyes of both beholders. Just as you cannot make other people love you, you cannot make them feel good about the way you choose to communicate with them. Discovering how to meet the needs of someone else when you interact often requires a delicate dance until you match your own footsteps with theirs. But it is never as simple as that. There also has to be a meeting of minds and a link from the hearts. Reaching a level that makes for comfortable satisfying communication with people close to you can take years, even a lifetime. Sadly, if we don’t practice them with each interaction, we too easily forget the steps and we have to relearn them again and again.
relationship can never be something one party feels and the other does not. It can be judged only in the eyes of both beholders. Just as you cannot make other people love you, you cannot make them feel good about the way you choose to communicate with them. Discovering how to meet the needs of someone else when you interact often requires a delicate dance until you match your own footsteps with theirs. But it is never as simple as that. There also has to be a meeting of minds and a link from the hearts. Reaching a level that makes for comfortable satisfying communication with people close to you can take years, even a lifetime. Sadly, if we don’t practice them with each interaction, we too easily forget the steps and we have to relearn them again and again.
We are all aware that uncontrolled stress can take a heavy toll on our health. It can precipitate heart attacks, suppress our immune system, rob us of rejuvenating restful sleep, and even shorten our lives. And there is nothing more stressful than unsatisfying communication with people who mean the most to us.
 No two human beings are alike. The needs they bring into a communication moment will never be the same. We’ve all known people we care about deeply who are so needy that it strains our powers to provide. Some spend their lives immersed in such insecurity and unexplained longing that you can never tell them often enough the affirmations they need to hear. No matter the number of times you praise some people, withhold it or disagree with them once, and you will have failed to meet their needs. Efforts to interact satisfactorily with those people can extract costs on the health of all parties concerned.
No two human beings are alike. The needs they bring into a communication moment will never be the same. We’ve all known people we care about deeply who are so needy that it strains our powers to provide. Some spend their lives immersed in such insecurity and unexplained longing that you can never tell them often enough the affirmations they need to hear. No matter the number of times you praise some people, withhold it or disagree with them once, and you will have failed to meet their needs. Efforts to interact satisfactorily with those people can extract costs on the health of all parties concerned.
Their constant state of unmet needs leads some to ceaselessly seek ways that they can prove their worth. The most common of these is to stake a claim on being “right.” Seldom is something so simple that someone can flip open a book and point to a passage and proclaim, “See. I was right.” Seldom are matters of fact at the heart of interpersonal disagreements. Shouldn’t you just agree to disagree and let it go? That is almost never satisfying communication among close friends and loved ones. Doing that leaves you to talk about things and people and the weather. The very feature that distinguishes an intimate relationship from one with a stranger is the freedom to express complex, sensitive thoughts. And express differences of opinion.
Few things in life are easily separated into two distinct categories: right or wrong. There is little satisfaction to be derived from being reminded of that. Butting heads with those you love will result in far fewer bruises, ego included, if you both understand some fundamental principles of persuasion. Clearly, speaking loudly does not sway minds. And even the softest ceaseless repetition will not help you prevail.
There are some steps that help increase mutual communication satisfaction. First, pick the right time and the right place to bring up touchy topics. Use qualifiers that make your words less bitter in case you have to eat them. “It  seems,” “Based on what I have read,” “Having dealt with this issue many times,” or simply, “My opinion on this issue is.” Declamations of certainty don’t invite open discussion. They don’t warmly welcome alternate views.
seems,” “Based on what I have read,” “Having dealt with this issue many times,” or simply, “My opinion on this issue is.” Declamations of certainty don’t invite open discussion. They don’t warmly welcome alternate views.
Pick one issue and stick to it. Mirror others’ objections. Work to understand them and see where common ground can be reached. It may require repeated efforts but don’t give up in pointing out genuine areas of agreement. If you feel the need to refer to your special knowledge of or experience with an issue, do so without fanfare and without expecting to rule because of it. The most inexpert among us can sometimes offer the most worthwhile, insightful observations.
Avoid attacking the person’s character with the claim that you are refuting his or her opinions. When you do, you will not only be side-stepping the real issue, you will be kindling a fire where there should have been nonthreatening illumination. Ask yourself, if I alienate someone close to my heart, what does it gain me to be right?
Some of us with well-developed social skills settle into a narrow relationship mode with selected others in our lives. Falling into predictable patterns may be partly due to meeting expectations and partly due to the ease of habit. You’ve experienced this behavior firsthand or witnessed it in others. Someone will be a jokester with one cousin and almost austere with another. Cordial with one aunt and curtly blunt with another. Open and receptive to differences with one sibling while leaning toward condescension with another.
Behaviors, based on what we think others believe about us or expect of us, can be adjusted. Though it takes two to establish such patterns, one of them can begin to change their static nature. What works well for many is to ask a simple question while showing genuine interest to hear the answer. “If you had to sum up your philosophy of life in ten words or so, what would you say it is?” The answer can enlighten you both and lift clouds away from a stifling or oppressive atmosphere.
Yet another strange anomaly is too common among intimates. Some people were born with repair kits in their hand. Their mission in life is to fix all the imperfect people they know. They see others as covered with lint and they can’t wait to start pick pick picking away. It can be a little help with our grammar. Or correcting those niggling little details in our stories we never get quite right. Especially annoying are those who assure all who will listen that we must be confused about our facts. Often these well-intentioned folks can be disarmed with a lengthy pause and a warm smile and a simple “Thank you. I’ll work on that.” Recognizing my leaning in this direction, I try to keep reminding myself that “It takes only a moment to notice in others what it takes a lifetime to see in ourselves.”
One of my most constant personal goals is to never stop learning, not only about topics of great interest to me but about the most mystifying subject of all: myself. Beyond that, I am committed to improve upon what I find when I look  deep inside every day. Few of us would deny the benefits to be derived from self study, self-improvement or the difficulty of sticking to this task. Even those of us who relish that challenge too often fail to see the need to do the same with others in our lives.
deep inside every day. Few of us would deny the benefits to be derived from self study, self-improvement or the difficulty of sticking to this task. Even those of us who relish that challenge too often fail to see the need to do the same with others in our lives.
How often do we interact with others on the false assumption that we know what they want to hear, what their needs are, what their immediate concerns are, even what they are thinking. As one philosopher warned, “When you try to read others’ minds and motives, you sometimes miss by inches, but mostly by miles.” Every satisfying encounter is a process of discovery, both about yourself and the one you would hope to impact, inform, impress, amuse, or persuade.
In intimate communication, the demands are even greater than in the world of casual conversation or the kind we rely on at work. The filters we use with close family and friends when we send and receive messages are fundamentally the same as those we use elsewhere: our experiences, our knowledge, our environment, our feelings, our needs, our biases, etc. But these filters have to be much more refined and focused in intimate communication.
All these filters affect the words we choose when we speak and the way we  interpret when we listen. We cannot ignore these filters if we hope to function as and be perceived as sensitive communicators. Yes, we have our facial and body expressions to aid us when we interact face-to-face. Actually, non-verbal carries the bulk of the weight in effective listening: touching, nodding, laughing, leaning, smiling, tone, volume, pitch, pauses and countless other little things. Too many people believe they have mastered the art of sensitive listening. Yet, it is one of the most prized and least developed skills on earth.
interpret when we listen. We cannot ignore these filters if we hope to function as and be perceived as sensitive communicators. Yes, we have our facial and body expressions to aid us when we interact face-to-face. Actually, non-verbal carries the bulk of the weight in effective listening: touching, nodding, laughing, leaning, smiling, tone, volume, pitch, pauses and countless other little things. Too many people believe they have mastered the art of sensitive listening. Yet, it is one of the most prized and least developed skills on earth.
When not face-to-face, our obligations to choose our words with care increase multi-fold. It is especially easy to get careless in this age of electronic media. It goes without saying that being clear is a challenge when we have no give and take. Selecting just the right words cannot be done without a view to the reader.
 Most important of all, when we write messages, we have to give careful consideration to the “tone” of the words we choose. Cocky and confident have similar meanings but are markedly different in tenor and tone. Connotations are built into countless words. In and of themselves, they can be negative, indifferent, condescending, hostile, or irreverent regardless of your intent. The possibilities are endless when it comes to the ways of skirting around saying someone is lying. We can refer to their stories, unsupported claims, or disingenuous declamations. My all-time favorite is “He is practiced in the artistry of shading the truth.”
Most important of all, when we write messages, we have to give careful consideration to the “tone” of the words we choose. Cocky and confident have similar meanings but are markedly different in tenor and tone. Connotations are built into countless words. In and of themselves, they can be negative, indifferent, condescending, hostile, or irreverent regardless of your intent. The possibilities are endless when it comes to the ways of skirting around saying someone is lying. We can refer to their stories, unsupported claims, or disingenuous declamations. My all-time favorite is “He is practiced in the artistry of shading the truth.”
Regardless of how short the written message, we must allow ourselves sufficient time to read and re-read it with a view as to not only whether it is clear, but how it will make the reader feel. Far too often, when we relate to close loved ones, we are least attentive to the kind of proofreading that matters most. Before excusing yourself by saying you were swamped and didn’t have enough time, think about the hours and days and even years it may take to make amends for something said in haste. I am reminded of my uncle’s clever poem about a speeder who ended up in an early grave: “But, oh, just think of the time he saved.”
As we age, we tend to limit our circle of close friends to those with whom we can have satisfying communication. That is wise. Dealing with family makes such decisions more difficult, but there are some whose world view and basic values are so opposed to our own, we may have to settle for infrequent, even superficial interaction, to save our sanity and avoid unnecessary stress.
We all know that love is not something to which we are entitled. It is something  we have to earn every day with word and deed. None of the intimate communication problems I have identified here are simple to correct. The factors that contribute to each are complex and multi-faceted. It is too easy to create a new problem in our attempt to eliminate another. That doesn’t mean we stop trying. The first thing we have to remember is that none of our interactions have a distinct and separate beginning and end. Relationships exist on a continuum that cannot be taken out of context and treated as independent events.
we have to earn every day with word and deed. None of the intimate communication problems I have identified here are simple to correct. The factors that contribute to each are complex and multi-faceted. It is too easy to create a new problem in our attempt to eliminate another. That doesn’t mean we stop trying. The first thing we have to remember is that none of our interactions have a distinct and separate beginning and end. Relationships exist on a continuum that cannot be taken out of context and treated as independent events.
The most fruitful approach is to begin by looking into the mirror. There we see the person closest to us over whom we have the greatest control. If you have to wonder, “Does this apply to me?” It probably does. The more successful we are in recognizing and improving on our own shortcomings when we relate to others the more changes we will begin to see in them. Therein lies the real power of effective interpersonal communication that contributes most profoundly to our own health and to that of the people most precious in our lives.
-0-
 An award winning high school speech and English teacher, Priscilla Diffie-Couch went on to get her ED.D. from Oklahoma State University, where she taught speech followed by two years with the faculty of communication at the University of Tulsa. In her consulting business later in Dallas, she designed and conducted seminars in organizational and group communication.
An award winning high school speech and English teacher, Priscilla Diffie-Couch went on to get her ED.D. from Oklahoma State University, where she taught speech followed by two years with the faculty of communication at the University of Tulsa. In her consulting business later in Dallas, she designed and conducted seminars in organizational and group communication.
An avid tennis player, she has spent the last twenty years researching and reporting on health for family and friends. She has two children, four grandchildren and lives with her husband Mickey in The Woodlands, Texas.
-0-
Bob Aronson has worked as a broadcast journalist, Minnesota Governor’s Communications Director and for 25 years led his own company as an international communication consultant specializing in health care.
In 2007 he had a heart transplant at the Mayo Clinic in Jacksonville, Florida. He is the Bob of Bob’s Newheart and the author of most of the nearly 300 posts on this site. He is also the founder of Facebook’s over 4,000 member Organ Transplant Initiative (OTI) support group.
You may comment in the space provided or email your thoughts to him at bob@baronson.org. And – please spread the word about the immediate need for more organ donors. There is nothing you can do that is of greater importance. If you convince one person to be an organ and tissue donor you may save or positively affect over 60 lives. Some of those lives may be people you know and love.
Mobility Scooters and Wheelchairs. Who Pays and Other Good Stuff
Nobody grows up obsessed with the idea of getting a mobility scooter or a wheelchair. They are not on anyone’s wish list unless your physical mobility is limited. While these means of transportation offer disabled people a new sense of freedom, they also bring some new and unexpected realities to life.
This blog is primarily about how to select a mobility scooter  and how to determine if Medicare will pay for it. At some future date I might focus on other issues important to the disabled.
and how to determine if Medicare will pay for it. At some future date I might focus on other issues important to the disabled.
You will likely find that my emphasis is on scooters and that’s only because they the most common and least expensive way to get from one place to another if walking is not an option. Also, I am a mobility scooter user. We may address motorized wheelchairs specifically later. There are, though, some commonalities both share. One thing is certain. Your life is in for some big changes once you accept the keys to your new ride.
 Scooter or wheelchair? That’s probably not a
Scooter or wheelchair? That’s probably not a decision you will have to make, your physical condition may dictate what will work best for you, Disabled World offers this explanation. (http://tinyurl.com/b4gxgl)
decision you will have to make, your physical condition may dictate what will work best for you, Disabled World offers this explanation. (http://tinyurl.com/b4gxgl)
Issues to Consider when Buying a Mobility Vehicle:
- Electric wheelchairs tend to be far more expensive than mobility scooters
- If you need to transport your personal mobility vehicle, a compact mobility scooter can be folded up to fit in a trunk or a back seat. Alternately, you can carry them behind a car with a trailer. Most electric wheelchairs do not fold and are too heavy for a simple trailer.
- If you have a wheelchair-modified van, it is easier and safer to tie down an electric wheelchair than a mobility scooter
- An electric medical scooter is steered with bicycle-like handlebars, whereas electric wheelchairs use a joystick. If you have issues with upper body mobility, a wheelchair might be easier to control.
- If you have posture issues, a wheelchair usually offers more features and support to help you, including motorized stand, tilt, and recline options.
- If you need to stay in your mobility aid for most of the day, a wheelchair is usually more comfortable.
The right choice of a personal mobility vehicle depends on how you are planning to use it.
- Are tight corners an issue?
- Would you like to fully enjoy the great outdoors, or are you more interested in shopping?
- Will you be running local errands, using public transportation, or using your own vehicle to move your personal mobility vehicle?
Once you answer these questions, you will be able to make the right choice for your specific situation.
I am the owner of two mobility scooters because I have COPD and can’t walk very far. One of the scooters is for outside the home and the other is for venues that offer flat, even surfaces upon which I can ride. Both of my scooters were paid for privately, no government funds were applied for or offered. If you want every minute detail about the process of acquiring mobility vehicles go to https://www.medicare.gov/coverage/manual-wheelchairs-and-power-mobility-devices.html If a summary will satisfy you read on.
 Let’s start with the most common question. “Will Medicare pay for my wheelchair or mobility scooter?” That single question is the cause of a lot of confusion, because the answer is, “Maybe.”
Let’s start with the most common question. “Will Medicare pay for my wheelchair or mobility scooter?” That single question is the cause of a lot of confusion, because the answer is, “Maybe.”
There are many suppliers who will tell you that Medicare will pay and you may even hear it from trusted friends. Here’s the truth. Medicare will pay up to 80% of the cost of an “approved” scooter or wheelchair if the supplier accepts Medicare assignment. That means they have to agree in writing that they will accept what Medicare will pay and you can be billed for no more than 20 percent of the total. If the supplier does not accept Medicare assignment Medicare will still pay the standard amount, but the supplier can send you a bill for any amount they choose.
So, back to the answer. For Medicare to pay for a manual  (unpowered) wheelchair, a senior must have a condition which prevents them from moving around in their home as they go about daily living. Their disability cannot be resolved through the use of a cane or walker and the wheelchair cannot be necessary only for use outside the home.
(unpowered) wheelchair, a senior must have a condition which prevents them from moving around in their home as they go about daily living. Their disability cannot be resolved through the use of a cane or walker and the wheelchair cannot be necessary only for use outside the home.
For Medicare to pay for an electric or powered wheelchair or scooter the individual must have the same needs as for a manual wheelchair but they must prove they do not have the physical strength to operate it. In addition they must demonstrate they have the ability to control the powered device without hurting themselves or those around them. Key point
here. You have to show that you need it to get around in your home and that your home is barrier free.
In either case, getting Medicare to pay is not an easy task. A written order from a doctor is necessary which must state the medical reason for the need and the type of wheelchair which is required. Be very careful. Medicare fraud is rampant and usually committed by suppliers or others who sell the goods, services, medicine and medical equipment that seniors need.
 Recently I met a man my age who had a scooter identical to mine. I asked how he liked it and he told me that not only was it a great scooter but that Medicare had paid for it. Now I know better than that so I asked how that worked and he explained that with the help of his scooter supplier he found a physician who provided the medical certification he needed. Beware – if any supplier has a list of Doctors you can see who will approve your purchase it is likely you will get one fraudulently.
Recently I met a man my age who had a scooter identical to mine. I asked how he liked it and he told me that not only was it a great scooter but that Medicare had paid for it. Now I know better than that so I asked how that worked and he explained that with the help of his scooter supplier he found a physician who provided the medical certification he needed. Beware – if any supplier has a list of Doctors you can see who will approve your purchase it is likely you will get one fraudulently.
The Medicare website says this about getting started on the road to acquiring a scooter or wheelchair. http://www.medicareinteractive.org/page2.php?topic=counselor&page=script&script_id=189
“Before you get your wheelchair or scooter, you must have an office visit with your doctor. The visit should take place no more than 45 days before the DME (Durable Medical Equipment) order and should deal with the medical reasons you need the wheelchair or scooter.
Your provider must sign an order or fill out a prescription or certificate that states that you need the power wheelchair or scooter to function in the home. The order must state:
Your health makes it very hard to move around in your home even with the help of a walker or cane;
- You have significant problems in your home performing activities of daily living such as getting to the toilet, getting in and out of a bed or a chair, bathing, and dressing;
- If you need a power wheelchair, you cannot use a manual wheelchair or scooter, but you can safely use a power wheelchair and
- The required office visit with your doctor took place.
The equipment must be necessary for you in the home but you can also use it outside the home. You can get only one piece of equipment to address your at-home mobility problem. Your doctor or other provider will determine what equipment you need based on your condition, what equipment can be used in your home, and what equipment you are able to use.”
Now some other scooter issues.
As we mentioned the scooter has to first be approved for use in your home. If that has been done then you must consider where else you might use it. Medicare might give you some leeway in your choice of vehicles, but not much and if they do and you choose one with all the bells and whistles you could wind up with a hefty bill.
Outside the home, here’s what you should consider.
- How will you transport it? Assuming you might want to
 pack it into the back of the mini-van how will you do that? Your scooter will have to be transportable, that means lightweight and easy to disassemble and assemble unless you can afford a power ramp on the back of your vehicle, one onto which you can drive so there’s no lifting or disassembling involved.
pack it into the back of the mini-van how will you do that? Your scooter will have to be transportable, that means lightweight and easy to disassemble and assemble unless you can afford a power ramp on the back of your vehicle, one onto which you can drive so there’s no lifting or disassembling involved. - How much clearance is there between the bottom of the scooter and the road below? My bigger scooter has a little over 5 inches. The new, smaller one has but 2.5. That means if you get into an area without curb cuts you will be unable to use sidewalks and take my word for it, the streets are no place for scooters or wheelchairs. They are much too slow and often invisible to drivers of cars and trucks. Smaller scooters with low clearance can get stopped by ruts, bumps and uneven surfaces very easily and if you are alone, what do you do?
- Lighting. Most scooters and wheelchairs don’t come with it. Buy a headlight and taillight anyway, you never know when you will be caught out after dark and a scooter or wheelchair without lights is an accident waiting to happen. Some mobility vehicles don’t even come with reflectors, buy a couple of those as well.
- Safety flag. You should also purchase a safety flag that
 stands about 4 or 5 feet high from the back of your vehicle. It will help both drivers and pedestrians see you coming and add some safety insurance.
stands about 4 or 5 feet high from the back of your vehicle. It will help both drivers and pedestrians see you coming and add some safety insurance. - A basket. Most come with a basket, but if not get one. You will need somewhere to put your “Stuff.” You can even buy drink holders that snap on to your armrests.
- Because I drive my scooter to the supermarket about a mile away a couple of times a week I drive though areas where homes are being remodeled or built and where other construction work is done. I had several flat tires until I went to a local bicycle shop to have solid rubber tires installed. No more flats. Some will tell you that solid rubber tires offer a much bumpier ride, but the fact is that scooters and wheelchairs ride like skate boards anyway. Get the solid rubber. If you are a purist and insist on pneumatic tires, get a patch kit and a tire pump and keep it in the basket of your scooter because you will need it.
- Cane holder. If you use a cane you’ll need a holder. The maker of your vehicle probably has them as an accessory or they might even include one at no extra charge.
- Rear View Mirror. It may sound silly but consider this, you are driving and you need to know what’s in back of you as well as what’s ahead. Rear view mirrors will come in quite handy. You will realize how important they are when you back into someone for the first time.
- Batteries. How far will they take you, how long will they last and do they come with a charger?
- Capacity. How much weight will it safely transport?
- Test drive. Ask to take it somewhere out of the showroom…around the block, into a mall, somewhere where you can get the “feel” of the scooter.
Those are the basics. I know I have only scratched the surface, but perhaps you will find something useful here anyway. You can add to the list once you have become an experienced mobility vehicle driver – and – you will add to the list. I purposely did not get into Scooter/Wheelchair brands and suppliers. Just Google Mobility scooters/wheelchairs and you will get all the information you need. There are also several Internet forums you can join to chat with other users about their experiences.
 Finally, this word. There have been admirable attempts at making the world more accessible, but they are too few and still too rare. In many buildings you will find stairways and no ramps. Disabled parking is often abused by those who don’t need it. Mobility carts in supermarkets and other businesses are wonderful, if you can get one. Again, too many people who don’t need them, ride them. Even the sidewalks can be problematic when cars parked in driveways overlap and block the sidewalk, forcing scooters and wheelchairs into the street. And, most importantly those of us who are disabled are simply not seen. I can’t tell you how many times people are looking over my head as they walk right into my scooter.
Finally, this word. There have been admirable attempts at making the world more accessible, but they are too few and still too rare. In many buildings you will find stairways and no ramps. Disabled parking is often abused by those who don’t need it. Mobility carts in supermarkets and other businesses are wonderful, if you can get one. Again, too many people who don’t need them, ride them. Even the sidewalks can be problematic when cars parked in driveways overlap and block the sidewalk, forcing scooters and wheelchairs into the street. And, most importantly those of us who are disabled are simply not seen. I can’t tell you how many times people are looking over my head as they walk right into my scooter.
Elevators also present a problem. If I can get my scooter in all  the way to the back of the elevator before anyone enters there is usually room for several more people and often they will stand back and allow me to do that. On other occasions, though, the crowd surges around me, packs the elevator and then as the door is closing they will look surprised when they see there is no room for me even though I was there first.
the way to the back of the elevator before anyone enters there is usually room for several more people and often they will stand back and allow me to do that. On other occasions, though, the crowd surges around me, packs the elevator and then as the door is closing they will look surprised when they see there is no room for me even though I was there first.
Anyone who has a mobility vehicle will have their own stories to tell. None of us want special treatment we only want to be noticed and considered. And, oh, there is one more item. Don’t be surprised when while on your scooter in the company of your significant other a clerk or salesperson will address them not you. For example it is not uncommon for a clerk who would like me to get up to look at something to say to my wife, “Can he walk?” She often says, “Yes, and he hears and talks, too.”
So, the next time you see a disabled person think for just a moment about what it must be like to be unable to walk very far if at all and how riding a scooter or wheelchair presents a whole new set of barriers. A little consideration goes a very long way.
I have written two other blogs on mobility vehicles here on Bob’s Newheart. You can find them by clicking on these links.
https://bobsnewheart.wordpress.com/2013/10/09/mobility-scooter-extended-test-drive-report/
https://bobsnewheart.wordpress.com/2013/07/10/mobility-scooters-a-first-time-users-observations/
-0-
 Bob Aronson of Bob’s Newheart is a 2007 heart transplant recipient, the founder of Facebook’s over 4,200 member Organ Transplant Initiative (OTI) and the author of most of these donation/transplantation blogs. You may comment in the space provided or email your thoughts to me at bob@baronson.org. And – please spread the word about the immediate need for more organ donors. There is nothing you can do that is of greater importance. If you convince one person to be an organ and tissue donor you may save or positively affect over 60 lives. Some of those lives may be people you know and love. You can register to be a donor at http://www.donatelife.net. It only takes a few minutes. Then, when registered, tell your family about your decision so there is no confusion when the time comes.
Bob Aronson of Bob’s Newheart is a 2007 heart transplant recipient, the founder of Facebook’s over 4,200 member Organ Transplant Initiative (OTI) and the author of most of these donation/transplantation blogs. You may comment in the space provided or email your thoughts to me at bob@baronson.org. And – please spread the word about the immediate need for more organ donors. There is nothing you can do that is of greater importance. If you convince one person to be an organ and tissue donor you may save or positively affect over 60 lives. Some of those lives may be people you know and love. You can register to be a donor at http://www.donatelife.net. It only takes a few minutes. Then, when registered, tell your family about your decision so there is no confusion when the time comes.
What You Need To Know About Your Liver and The Transplant Process
By Bob Aronson
 The liver is an incredibly important organ and the only one in the human body that can regenerate itself. It is second only in size to the skin (yes the skin is an organ) and has been described as boomerang shaped. Virtually every nutrient we consume passes through the liver so it can be processed and turned into a different biochemical form for use by other organs.
The liver is an incredibly important organ and the only one in the human body that can regenerate itself. It is second only in size to the skin (yes the skin is an organ) and has been described as boomerang shaped. Virtually every nutrient we consume passes through the liver so it can be processed and turned into a different biochemical form for use by other organs.
Located just below the rib cage in the upper right side of your abdomen the liver has three main functions. It helps in digestion makes proteins and helps eliminate toxic substances.
The liver is the only organ in the body that can easily replace damaged cells, but if enough cells are lost, the liver may not be able to meet the needs of the body.
The liver is like a very complex factory. Included in its many functions are: http://www.medicinenet.com/liver_anatomy_and_function/images-quizzes/index.htm
- Production of bile that is required in the digestion of food, in particular fats;
- Storing of the extra glucose or sugar as glycogen, and then converting it back into glucose when the body needs it for energy;
- Production of blood clotting factors;
- Production of amino acids (the building blocks for making proteins), including those used to help fight infection;
- The processing and storage of iron necessary for red blood cell production;
- Manufacture of cholesterol and other chemicals required for fat transport;
- Conversion of waste products of body metabolism into urea that is excreted in the urine; and
- Metabolizing medications into their active ingredient in the body.
- Cirrhosis is a term that describes permanent scarring of the liver. In cirrhosis, the normal liver cells are replaced by scar tissue that cannot perform any liver function.
- Acute liver failure may or may not be reversible, meaning that on occasion, there is a treatable cause and the liver may be able to recover and resume its normal functions.
The Liver can be affected by any one of a number of diseases. Click on the item of interest in the list below for a complete explanation.
The Liver Disease Information Center provides information on a variety of topics related to liver health and 
liver disease. http://www.liverfoundation.org/abouttheliver/info/
- Alagille Syndrome
- Alcohol-Related Liver Disease
- Alpha-1 Antitrypsin Deficiency
- Autoimmune Hepatitis
- Benign Liver Tumors
- Biliary Atresia
- Cirrhosis
- Clinical Trials
- Galactosemia
- Gilbert Syndrome
- Hemochromatosis
- Hepatitis A
- Hepatitis B
- Hepatitis C
- Hepatocellular Carcinoma
- Hepatic Encephalopathy
- Liver Biopsy
- Liver Cysts
- Liver Cancer
- Liver Function Tests
- Liver Transplant
- Newborn Jaundice
- Non-Alcoholic Fatty Liver Disease
- Primary Biliary Cirrhosis (PBC)
- Primary Sclerosing Cholangitis (PSC)
- The Progression of Liver Disease
- Reye Syndrome
- Type I Glycogen Storage Disease
- Wilson Disease
- Intrahepatic Cholestasis of Pregnancy (ICP)
How does alcohol affect the liver? (From the American Liver Foundation) http://www.liverfoundation.org/abouttheliver/info/alcohol/
Alcohol can damage or destroy liver cells.
 The liver breaks down alcohol so it can be removed from your body. Your liver can become injured or seriously damaged if you drink more alcohol than it can process.
The liver breaks down alcohol so it can be removed from your body. Your liver can become injured or seriously damaged if you drink more alcohol than it can process.
What are the different types of alcohol-related liver disease?
There are three main types of alcohol-related liver disease: alcoholic fatty liver disease, alcoholic hepatitis, and alcoholic cirrhosis.
Alcoholic fatty liver disease
Alcoholic fatty liver disease results from the deposition of fat in liver cells. It is the earliest stage of alcohol-related liver disease. There are usually no symptoms. If symptoms do occur, they may include fatigue, weakness, and discomfort localized to the right upper abdomen. Liver enzymes may be elevated, however tests of liver function are often normal. Many heavy drinkers have fatty liver disease. Alcoholic fatty liver disease may be reversible with abstinence of alcohol.
Alcoholic hepatitis
Alcoholic hepatitis is characterized by fat deposition in liver cells, inflammation and mild scarring of the liver. Symptoms may include loss of appetite, nausea, vomiting, abdominal pain, fever and jaundice. Liver enzymes are elevated and tests of liver function may be abnormal. Up to 35 percent of heavy drinkers develop alcoholic hepatitis and of these 55% already have cirrhosis.
Alcoholic hepatitis can be mild or severe. Mild alcoholic hepatitis may be reversed with abstinence. Severe alcoholic hepatitis may occur suddenly and lead to serious complications including liver failure and death.
Alcoholic cirrhosis
Alcoholic cirrhosis, the most advanced type of alcohol induced liver injury is characterized by severe scarring and disruption of the normal structure of the liver — hard scar tissue replaces soft healthy tissue. Between 10 and 20 percent of heavy drinkers develop cirrhosis. Symptoms of cirrhosis may be similar to those of severe alcoholic hepatitis. Cirrhosis is the most advanced type of alcohol-related liver disease and is not reversed with abstinence. However, abstinence may improve the symptoms and signs of liver disease and prevent further damage
The Liver Transplant
Liver transplants are performed only for patients with end-stage liver disease for whom standard medical and surgical therapies have failed. Conditions that can lead to liver transplantation include:  (http://www.barnesjewish.org/conditions-leading-to-liver-transplant)
(http://www.barnesjewish.org/conditions-leading-to-liver-transplant)
- Cirrhosis: cryptogenic, alcoholic, autoimmune, hepatitis B, hepatitis C, fatty liver disease (NASH)
- Hepatocellular carcinoma (liver cancer)
- Primary sclerosing cholangitis (disease of the liver bile ducts)
- Primary biliary cirrhosis (PBC – bile ducts in the liver slowly deteriorate)
- Alpha-1-antitrypsin deficiency (genetic disorder leading to abnormal amounts of A1AT protein in liver cells)
- Acute liver failure
- Cholangiocarcinoma (bile duct cancer)
- Wilson’s disease
Liver transplants are the second most common transplants after kidneys. They require that the blood type and body size of the donor match the person receiving the new organ. There are more 6,000 liver transplants are performed each year in the United States. The surgery usually takes between four and twelve hours and most patients can expect a hospital stay of up to three weeks following surgery. . .
Essential Information For The Transplant Patient
Most transplant centers function in pretty much the same manner, but Johns Hopkins Medical Center in Baltimore, Maryland offers one of the best summaries of what the transplant patient can expect. http://www.hopkinsmedicine.org/healthlibrary/test_procedures/gastroenterology/liver_transplantation_procedure_92,P07698/
Risks of the procedure
As with any surgery, complications can occur. Some complications from liver transplantation may include, but are not limited to, the following:
- Bleeding
- Infection
- Blockage of the blood vessels to the new liver
- Leakage of bile or blockage of bile ducts
- Initial lack of function of new liver
The new liver may not function for a brief time after the transplant. The new liver may also be rejected. Rejection is a normal reaction of the body to a foreign object or tissue. When a new liver is transplanted into a recipient’s body, the immune system reacts to what it perceives as a threat and attacks the new organ, not realizing that the transplanted liver is beneficial. To allow the organ to survive in a new body, medications must be taken to trick the immune system into accepting the transplant and not attacking it as a foreign object.
Contraindications for liver transplantation include, but are not limited to, the following:
- Current or recurring infection that cannot be treated effectively
- Metastatic cancer. This is cancer that has spread from its primary location to one or more additional locations in the body.
- Severe cardiac or other medical problems preventing the ability to tolerate the surgical procedure
- Serious conditions other than liver disease that would not improve after transplantation
- Noncompliance with treatment regimen
- Alcohol consumption
There may be other risks depending on your specific medical condition. Be sure to discuss any concerns with your doctor prior to the procedure.
Before the procedure
In order to receive a liver from an organ donor who has died (cadaver), a recipient must be placed on a waiting list of the United Network for Organ Sharing (UNOS). Extensive testing must be done before an individual can be placed on the transplant list.
Because of the wide range of information necessary to determine eligibility for transplant, the evaluation process is carried out by a transplant team. The team includes a transplant surgeon, a transplant hepatologist (doctor specializing in the treatment of the liver), one or more transplant nurses, a social worker, and a psychiatrist or psychologist. Additional team members may include a dietitian, a chaplain, and/or an anesthesiologist.
Components of the transplant evaluation process include, but are not limited to, the following:
- Psychological and social evaluation. Psychological and social issues involved in organ transplantation, such as stress, financial issues, and support by family and/or significant others are assessed. These issues can significantly impact the outcome of a transplant.
- Blood tests. Blood tests are performed to help determine a good donor match, to assess your priority on the donor list, and to help improve the chances that the donor organ will not be rejected.
- Diagnostic tests. Diagnostic tests may be performed to assess your liver as well as your overall health status. These tests may include X-rays, ultrasound procedures, liver biopsy, and dental examinations. Women may receive a Pap test, gynecology evaluation, and a mammogram.
The transplant team will consider all information from interviews, your medical history, physical examination, and diagnostic tests in determining your eligibility for liver transplantation.
Once you have been accepted as a transplant candidate, you will be placed on the UNOS list. Candidates in most urgent need of a transplant are given highest priority when a donor liver becomes available based on UNOS guidelines. When a donor organ becomes available, you will be notified and told to come to the hospital immediately.
If you are to receive a section of liver from a living family member (living-related transplant), the transplant may be performed at a planned time. The potential donor must have a compatible blood type and be in good health. A psychological test will be conducted to ensure the donor is comfortable with the decision.
The following steps will precede the transplant:
- Your doctor will explain the procedure to you and offer you the opportunity to ask any questions about the procedure.
- You will be asked to sign a consent form that gives your permission to do the surgery. Read the form carefully and ask questions if something is not clear.
- For a planned living transplant, you should fast for eight hours before the operation, generally after midnight. In the case of a cadaver organ transplant, you should begin to fast once you are notified that a liver has become available.
- You may receive a sedative prior to the procedure to help you relax.
- Based on your medical condition, your doctor may request other specific preparation.
During the procedure
Liver transplantation requires a stay in a hospital. Procedures may vary depending on your condition and your doctor’s practices.
Generally, a liver transplant follows this process:
- You will be asked to remove your clothing and given a gown to wear.
- An intravenous (IV) line will be started in your arm or hand. Additional catheters will be inserted in your neck and wrist to monitor the status of your heart and blood pressure, as well as for obtaining blood samples. Alternate sites for the additional catheters include the subclavian (under the collarbone) area and the groin.
- You will be positioned on the operating table, lying on your back.
- If there is excessive hair at the surgical site, it may be clipped off.
- A catheter will be inserted into your bladder to drain urine.
- After you are sedated, the anesthesiologist will insert a tube into your lungs so that your breathing can be controlled with a ventilator. The anesthesiologist will continuously monitor your heart rate, blood pressure, breathing, and blood oxygen level during the surgery.
- The skin over the surgical site will be cleansed with an antiseptic solution.
- The doctor will make a slanting incision just under the ribs on both sides of the abdomen. The incision will extend straight up for a short distance over the breast bone.
- The doctor will carefully separate the diseased liver from the surrounding organs and structures.
- The attached arteries and veins will be clamped to stop blood flow into the diseased liver.
- Depending on several factors, including the type of transplant being performed (whole liver versus a portion of liver), different surgical techniques may be used to remove the diseased liver and implant the donor liver or portion of the liver.
- The diseased liver will be removed after it has been cut off from the blood vessels.
- The doctor will visually inspect the donor liver or portion of liver prior to implanting it.
- The donor liver will be attached to the blood vessels. Blood flow to the new liver will be established and then checked for bleeding at the suture lines.
- The new liver will be connected to the bile ducts.
- The incision will be closed with stitches or surgical staples.
- A drain may be placed in the incision site to reduce swelling.
- A sterile bandage or dressing will be applied.
After the procedure In the hospital
After the surgery you may be taken to the recovery room before being taken to the intensive care unit (ICU) to be closely monitored for several days. Alternately, you may be taken directly to the ICU from the operating room. You will be connected to monitors that will constantly display your EKG tracing, blood pressure, other pressure readings, breathing rate, and your oxygen level. Liver transplant surgery requires an in-hospital stay of seven to 14 days, or longer.
You will most likely have a tube in your throat so that your breathing can be assisted with a ventilator until you are stable enough to breathe on your own. The breathing tube may remain in place for a few hours up to several days, depending on your situation.
You may have a thin plastic tube inserted through your nose into your stomach to remove air that you swallow. The tube will be removed when your bowels resume normal function. You will not be able to eat or drink until the tube is removed.
Blood samples will be taken frequently to monitor the status of the new liver, as well as other body functions, such as the kidneys, lungs, and blood system.
You may be on special IV drips to help your blood pressure and your heart and to control any problems with bleeding. As your condition stabilizes, these drips will be gradually weaned down and turned off as tolerated.
Once the breathing and stomach tubes have been removed and your condition has stabilized, you may start liquids to drink. Your diet may be gradually advanced to more solid foods as tolerated.
Your immunosuppression (antirejection) medications will be closely monitored to make sure you are receiving the optimum dose and the best combination of medications.
When your doctor feels you are ready, you will be moved from the ICU to a room on a regular nursing unit or transplant unit. Your recovery will continue to progress here. Your activity will be gradually increased as you get out of bed and walk around for longer periods of time. Your diet will be advanced to solid foods as tolerated.
Nurses, pharmacists, dietitians, physical therapists, and other members of the transplant team will teach you how to take care of yourself once you are discharged from the hospital.
At home
Once you are home, it will be important to keep the surgical area clean and dry. Your doctor will give you specific bathing instructions. The stitches or surgical staples will be removed during a follow-up office visit, if they were not removed before leaving the hospital.
You should not drive until your doctor tells you to. Other activity restrictions may apply.
Notify your doctor to report any of the following:
- This may be a sign of rejection or infection.
- Redness, swelling, or bleeding or other drainage from the incision site
- Increase in pain around the incision site. This may be a sign of infection or rejection.
- Vomiting and/or diarrhea
Your doctor may give you additional or alternate instructions after the procedure, depending on your particular situation.
What is done to prevent rejection?
To allow the transplanted liver to survive in a new body, you will be given medications for the rest of your  life to fight rejection. Each person may react differently to medications, and each transplant team has preferences for different medications.
life to fight rejection. Each person may react differently to medications, and each transplant team has preferences for different medications.
New antirejection medications are continually being developed and approved. Doctors tailor medication regimes to meet the needs of each individual patient.
Usually several antirejection medications are given initially. The doses of these medications may change frequently, depending on your response. Because antirejection medications affect the immune system, people who receive a transplant will be at higher risk for infections. A balance must be maintained between preventing rejection and making you very susceptible to infection.
Some of the infections you will be especially susceptible to include oral yeast infection (thrush), herpes, and respiratory viruses. You should avoid contact with crowds and anyone who has an infection for the first few months after your surgery.
The following are the most common symptoms of rejection. However, each individual may experience symptoms differently. Symptoms may include, but are not limited to, the following:
- Fever
- A yellowing of the skin and eyes due to bile pigments in the blood.
- Dark urine
- Itching
- Abdominal swelling or tenderness
- Fatigue or irritability
- Headache
- Nausea
The symptoms of rejection may resemble other medical conditions or problems. Consult your transplant teaoncerns you have. Frequent visits to and contact with the transplant team are essential.
Organ transplants are expensive and the cost goes well beyond the surgery itself. If you are told you need a transplant and are sent to a transplant center for evaluation you can bet one of the first questions you will be asked is, “Do you have the financial resources to pay for your transplant?”
According to the National Foundation for Transplants http://www.transplants.org/faq/how-much-does-transplant-cost the average cost of a liver transplant and first year expenses in the United States is $575,000.
The Mayo Clinic developed this helpful list of questions that will help you develop the answer to that question. http://www.mayoclinic.org/departments-centers/transplant-center/liver-transplant/choosing-mayo-clinic/costs-insurance-information
Insurance information
Before your transplant, it’s important that you work closely with your insurance company to understand your benefit plan. You’ll be responsible for any of your transplant and medical care costs not covered by your insurance company.
You may want to ask your insurance company several questions regarding your transplant expenses, including:
- What is the specific coverage of my plan? What are my deductibles, coinsurance, copayments, lifetime maximum amount and annual maximum amounts for both medical care and transplant services?
- Does my plan have a pre-existing or waiting period clause? If so, what is the time frame? Can this be waived?
- Does my plan include pharmacy coverage? If so, will my plan cover my current medications and immunosuppressant medications?
- Does my plan require any special approvals for evaluation or transplant? How long does the approval process take once submitted to insurance?
- Does my plan cover my transportation and lodging expenses during my transplant care?
- Does my current insurance require enrollment in Medicare when eligible?
- Does my insurance follow Medicare Coordination of Benefits guidelines?
- How will my current coverage change after enrolling in Medicare? Will my plan become a supplemental or secondary plan?
If your plan is a Medicare supplement, ask questions including:
- Does my plan follow Medicare guidelines?
- Does my plan cover Medicare Part A and B deductible and coinsurance?
- Does my plan have a pre-existing or waiting period? If so, what is the time frame?
- Does my plan offer an option for Medicare Part D coverage?
Other expenses
Please plan for other expenses that may occur related to your transplant, which may include follow-up medical appointments, long-term medications, caregiver expenses, travel, parking, lodging and other expenses.
Financial Aid
If you need an organ transplant, but don’t have the financial resources to pay for it you should first work with the transplant center social worker to see what is available. There are a number of resources for which you may qualify. Just click on this link for the complete list and explanation of services. http://www.transplantliving.org/before-the-transplant/financing-a-transplant/directory/
 Bob Aronson of Bob’s Newheart is a 2007 heart transplant recipient, the founder of Facebook’s over 4,200 member Organ Transplant Initiative (OTI) and the author of most of these donation/transplantation blogs. You may comment in the space provided or email your thoughts to me at bob@baronson.org. And – please spread the word about the immediate need for more organ donors. There is nothing you can do that is of greater importance. If you convince one person to be an organ and tissue donor you may save or positively affect over 60 lives. Some of those lives may be people you know and love. You can register to be a donor at http://www.donatelife.net. It only takes a few minutes.
Bob Aronson of Bob’s Newheart is a 2007 heart transplant recipient, the founder of Facebook’s over 4,200 member Organ Transplant Initiative (OTI) and the author of most of these donation/transplantation blogs. You may comment in the space provided or email your thoughts to me at bob@baronson.org. And – please spread the word about the immediate need for more organ donors. There is nothing you can do that is of greater importance. If you convince one person to be an organ and tissue donor you may save or positively affect over 60 lives. Some of those lives may be people you know and love. You can register to be a donor at http://www.donatelife.net. It only takes a few minutes.
How to Get the Most Bang for Your Prescription Medicine Buck
By Bob Aronson
 I am a senior citizen, who has had a heart transplant and who also has Chronic Obstructive Pulmonary Disease (COPD). I take a good number of prescription drugs and despite having Medicare Part D insurance I still pay thousands of dollars a year for my prescriptions. Most of the drugs I take have been around for quite a while, but not long enough to allow the sale of generics and because there are few if any pricing restrictions, most of my meds are outrageously high priced.
I am a senior citizen, who has had a heart transplant and who also has Chronic Obstructive Pulmonary Disease (COPD). I take a good number of prescription drugs and despite having Medicare Part D insurance I still pay thousands of dollars a year for my prescriptions. Most of the drugs I take have been around for quite a while, but not long enough to allow the sale of generics and because there are few if any pricing restrictions, most of my meds are outrageously high priced.
One of the drugs I take is called Foradil. It was approved by the FDA in February 2001 for the maintenance treatment of asthma and the prevention of bronchospasm in reversible obstructive airways disease.. Despite being on the market that long, it still retails for about $250.00 for a 30 day supply. Spiriva is another COPD drug and is often taken with Foradil. It retails for about $350.00. I take about a dozen drugs and these two alone total over $600.00 a month. Insurance cuts that cost in half, but they are still expensive. Because of these prices I know of many seniors and others who have to choose between eating and paying for their prescription meds.
It is an unfortunate fact of life that prescription drugs are more expensive in America than any other place in the world and as a result if you contract a serious illness like cancer you may not be able to afford the treatment that can save your life, even if you are insured.
It costs a whole lot of money to be sick in this country and a whole lot of people die — not because there is no medicine or treatment but because they can’t afford to get well. That strikes me as being just plain wrong.
no medicine or treatment but because they can’t afford to get well. That strikes me as being just plain wrong.
Healthcare costs are skyrocketing, but prescription drugs lead the parade. Americans now spend a staggering $200 billion a year on them and the end is nowhere in sight. The cost of staying alive is growing at the rate of about 12 percent a year. It appears as though people are taking a lot more drugs than they used to and they are taking the really expensive new ones instead of older, cheaper drugs. The reason? Either physicians are pushing new medications too hard or, more likely, people are seeing the ads for new drugs in the media and are demanding them. Strangely, unlike most other businesses where prices come down with time, that’s not true with drugs. Price increases are commonplace even with the older ones and the increases aren’t one time adjustments. Often the price tag increases several times a year.
Earlier I pointed out that Americans pay more for their drugs than any other country in the world — but it isn’t just a little more…it’s a whole lot. On average, the cost of prescription drugs in the U.S. is at least double what people in other countries pay for the same exact prescription and it some cases it is 10 times more.
A 2013 report from the International Federation of Health Plans, says Nexium, the pill commonly prescribed for acid reflux, costs U.S. patients more than $200, while Swiss citizens only pay $60 and people who live in the Netherlands pay $23. But Nexium is a drop in the bucket compared to cancer drugs. http://www.drugwatch.com/2014/10/15/americans-pay-higher-prces-prescription-drugs/
Not long ago CBS’ 60 Minutes devoted a segment to the absurdly high cost of cancer drugs. Correspondent Lesley Stahl reported that many cancer drugs cost well over $100,000 for a year’s worth of medicine. She said that in the fight against cancer, most people can expect to be on more than one drug. The bill for medications can escalate to nearly $300,000, a price tag that doesn’t include fees charged by a doctor or a hospital. Health insurance companies – including government polices like Medicare – don’t cover the full cost of these drugs. Some policies don’t cover some of these drugs at all.  But cancer is not alone in the extreme price arena. Drugs for chronic diseases like multiple sclerosis also carry inflated prices. Prescriptions of Copaxone and Gilenya cost about $4,000 and $5,500, respectively and that amount is almost three times more than the most-expensive price in other countries.
But cancer is not alone in the extreme price arena. Drugs for chronic diseases like multiple sclerosis also carry inflated prices. Prescriptions of Copaxone and Gilenya cost about $4,000 and $5,500, respectively and that amount is almost three times more than the most-expensive price in other countries.
In the case of almost every other product sold on the free market, the older a product gets the less it costs. In the case of cancer drugs in America, the inverse is actually true. Novartis developed Gleevec, one of the most popular cancer drugs, in 2001 and sold it for $28,000 a year. By 2012, its cost rose to $92,000. Despite not being a novel treatment, Novartis is allowed to hike up the price every year in the United States.
So If you are a reasonably intelligent person you will ask three questions. 1) Why do these drugs cost so much? 2) What is being done to bring the prices down? And 3) Is there help available to people who can’t afford the drugs that can keep them alive.
Let’s answer the questions one at a time. First. Why are drugs so expensive? Well, if you listen to the big pharma companies they will tell you that the cost reflects their investment in research and development of the drugs. They will tell you they spend millions on drugs that don’t pan out and that expense is passed on to the patient. But are they telling the truth? No they aren’t! Pharmaceutical companies are fond of saying Americans take the lion’s share of the R&D costs for the rest of the world – calling other countries “foreign free riders.” So, drug companies are forced to charge Americans more to recover what they don’t get from other countries.
pharma companies they will tell you that the cost reflects their investment in research and development of the drugs. They will tell you they spend millions on drugs that don’t pan out and that expense is passed on to the patient. But are they telling the truth? No they aren’t! Pharmaceutical companies are fond of saying Americans take the lion’s share of the R&D costs for the rest of the world – calling other countries “foreign free riders.” So, drug companies are forced to charge Americans more to recover what they don’t get from other countries.
In fact, the more disturbing truth is that companies charge what they want in the U.S., and it’s a profiteering paradise for them. U.S. law protects these companies from free-market competition. For example, Medicare is not allowed to negotiate prices. By law, it has to pay exactly what the drug companies charge for any drug. In effect our lawmakers told the pharmaceutical companies that they can charge whatever they want and we (the taxpayers) will pay it. Even may insurance companies don’t negotiate or do it half-heartedly. Companies make billions on most of these drugs, and they receive massive tax breaks for R&D, leading to inflated figures. Another huge portion of the costs are subsidized by taxpayers.
Here’s the sad part of all this R and D and the introduction of new drugs. Only 1 in 10 of them actually provides substantial benefit over old drugs. To add insult to injury the side effects of the new entries create the need for more drugs. And — some of these drugs have horrible complications that result in lawsuits to recover damages.
University of Medicine and Dentistry of New Jersey Health professor and policy expert Donald W. Light says, “We can find no evidence to support the widely believed claims from industry that lower prices in other industrialized countries do not allow companies to recover their R&D costs so they have to charge Americans more to make up the difference and pay for these ‘foreign free riders,’”
In contrast, governments in other countries put caps on the price of drugs and negotiate prices based on what the actual therapeutic benefit is. And Big Pharma still turns a healthy profit in other countries, despite costs being 40 percent lower than they are in the United States.
Big Pharma would have many Americans believe that it is disadvantaged by the costs of developing a new drug. The truth is, drug companies are far from impoverished. EvaluatePharma’s most recent report shows that 2013 was the biggest year since 2009 for drug approvals. These new drugs will add nearly $25 billion to Big Pharma’s coffers by 2018, and prescription drug sales will exceed one trillion dollars by 2020.
The health care industry as a whole has more than enough money, with billions left to continue pursuing its interests in Washington.
Big Pharma Spends More on Lobbying Than Anyone
 Since 1998, the industry spent more than $5 billion on lobbying in Washington, according to the Center for Responsive Politics. To put that in context, that’s more than the $1.53 billion spent by the defense industry and more than the $1.3 billion forked out by Big Oil.
Since 1998, the industry spent more than $5 billion on lobbying in Washington, according to the Center for Responsive Politics. To put that in context, that’s more than the $1.53 billion spent by the defense industry and more than the $1.3 billion forked out by Big Oil.
From 1998 to 2013, Big Pharma spent nearly $2.7 billion on lobbying expenses — more than any other industry and 42 percent more than the second highest paying industry: insurance. And since 1990, individuals, lobbyists and political action committees affiliated with the industry have doled out $150 million in campaign contributions.
The world’s 11 largest drug companies made a net profit of $711.4 billion from 2003 to 2012. Six of these companies are headquartered in the United Sates: Johnson & Johnson, Pfizer, Abbot Laboratories, Merck, Bristol-Myers Squibb and Eli Lilly. In 2012 alone, the top 11 companies earned nearly $85 billion in net profits. According to IMS Health, a worldwide leader in health care research, the global market for pharmaceuticals is expected to top $1 trillion in sales by 2014.http://www.drugwatch.com/manufacturer/
But the large amount of cash Big Pharma bestows on government representatives and regulatory bodies is small when compared with the billions it spends each year on direct-to-consumer advertising. In 2012, the industry invested nearly $3.5 billion into marketing drugs on the Internet, TV, radio and other outlets. The United States is one of only two countries in the world whose governments allow prescription drugs to be advertised on TV (the other is New Zealand).
industry invested nearly $3.5 billion into marketing drugs on the Internet, TV, radio and other outlets. The United States is one of only two countries in the world whose governments allow prescription drugs to be advertised on TV (the other is New Zealand).
A single manufacturer, Boehringer Ingelheim, spent $464 million advertising its blood thinner Pradaxa in 2011. The following year, the drug passed the $1 billion sales mark. The money in this business appears to be well-spent.
No sane person can object to a company making a profit, it’s part of the American way, but the drug industry’s profits are excessive. We paysignificantly more than any other country for the exact same drugs. Per capita drug spending in the U.S. is about 40 percent higher than Canada, 75 percent greater than in Japan and nearly triple the amount spent in Denmark.
So you might ask, “What can I do to get the lowest possible price for my prescriptions?” Well, there are a few things. You can shop for the best price and because of the internet that’s become a whole lot easier. You can look up a specific drug and find the best price at a pharmacy near you. Here are two resources, I’m sure you can find a lot more https://www.lowestmed.com/Search#/ or http://www.goodrx.com/ All; you  have to do is type in the drug you need and your zip code and it will find the price of that drug in pharmacies near you.
have to do is type in the drug you need and your zip code and it will find the price of that drug in pharmacies near you.
Transplant recipients might be interested in the cost of anti-rejection drugs. The price is hard to stomach but easy to find. In my zip code 32244 100 Mg Cyclosporine capsules range jn price from $526.00 at Wal Mart to $584 at Target. If you are a heart pateint and take Carvedilol in my neighborhood it ranges from $4.00 at WalMart to $9.54 at Kmart . Lisinopril also has a wide range. At the Publix Supermarket pharmacy near me it is FREE…that’s right FREE. But at CVS it is $12.00. Those price variations might make it worth a little longer drive to get a better bargain.
You can also get help with coupons which are an obvious choice to save money when grocery or clothes shopping, but they’re often overlooked as a way to cut costs of over-the-counter and prescription drugs. Manufactures frequently offer one time and repeat coupons that can save consumers hundreds of dollars on their medicines. “For our family it has been incredibly effective [in saving money] for a number of regular prescriptions,” says Stephanie Nelson, founder of the coupon website CouponMom.com.
The costs of prescription drugs and over-the-counter medications have been steadily rising and patients facing tight budgets are often forced to make hard decisions when it comes to what they can afford.
The savings vary by manufacturer, but according to Nelson, many companies offer discounts at each prescription refill while others offer discount cards that take $20 off co-pays. Others offer one-time coupons to cover the first use of a drug.
Consumer Reports Magazine says that there are other ways to save money, too. Whichever drugstore or pharmacy you use, choosing generics over brand-name drugs will save you money. Talk to your doctor, who may be able to prescribe lower-cost alternatives in the same class of drug. In addition, follow these tips.
- Request the lowest price.Our analysis showed that shoppers didn’t always receive the lowest
 available price when they called the pharmacy. Sometimes they were given a discounted price, and other times they were quoted the list price. Be sure to explain—whether you have insurance or not—that you want the lowest possible price. Our shoppers found that student and senior discounts may also apply, but again, you have to ask.
available price when they called the pharmacy. Sometimes they were given a discounted price, and other times they were quoted the list price. Be sure to explain—whether you have insurance or not—that you want the lowest possible price. Our shoppers found that student and senior discounts may also apply, but again, you have to ask. - Leave the city.Grocery-store pharmacies and independent drugstores sometimes charge higher prices in urban areas than in rural areas. For example, our shoppers found that for a 30-day supply of generic Actos, an independent pharmacy in the city of Raleigh, N.C., charged $203. A store in a rural area of the state sold it for $37.
- Get a refill for 90 days, not 30 days.Most pharmacies offer discounts on a three-month supply.
- Consider paying retail.At Costco, the drugstore websites, and a few independents, the retail prices were lower for certain drugs than many insurance copays.
- Look for additional discounts.All chain and big-box drugstores offer discount generic-drug programs, with some selling hundreds of generic drugs for $4 a month or $10 for a three-month supply. Other programs require you to join to get the discount. (Restrictions apply and certain programs charge annual fees.)
- Consumer Reports goes on to say that “although the low costs we found at a few stores could entice you to get your prescriptions filled at multiple pharmacies based only on price, our medical consultants say it’s best to use a single pharmacy. That keeps all of the drugs you take in one system, which can help you avoid dangerous drug interactions.”

Finally, what do you do if you’ve done the shopping, used coupons, followed all of the Consumer Report Tips and are still unable to pay for your prescriptions. Well, there is some limited assistance. Here are some resources.
-0-
Bob Aronson of Bob’s Newheart is a 2007 heart transplant recipient, the founder of Facebook’s over 4,200 member Organ Transplant Initiative (OTI) and the author of most of these donation/transplantation blogs. You may comment in the space provided or email your thoughts to me at bob@baronson.org. And – please spread the word about the immediate need for more organ donors. There is nothing you can do that is of greater importance. If you convince one person to be an organ and tissue donor you may save or positively affect over 60 lives. Some of those lives may be people you know and love. You can register to be a donor at http://www.donatelife.net. It only takes a few minutes.
People Who Say they Can’t Quit Smoking Are Gutless Liars!
By Bob Aronson…former smoker

if that headline doesn’t get your attention I don’t know what will.
“I can’t quit smoking,” is BS. You can quit, but you are a pansy, no guts. You can spread that “Can’t quit” manure elsewhere. It doesn’t work here because it’s a big lie.
Do I have your attention?
This post is aimed at smokers, whether you are just starting the habit or have smoked for a while and are thinking about quitting. I am writing this to alert you to smoking related issues not to draw attention to myself or my condition. I seek no sympathy nor attention.
Yes, this is a posting that encourages you to ignore the temptation to start smoking and/or to quit smoking if you already have the habit. In the interest of full disclosure let me tell you why you should read this. You should do so because I offer hope and straight talk. No one could possibly have had a greater addiction to cigarettes than I did. And…I know about addiction, too. Not only did I quit smoking (1991) I also quit drinking (1982) after years as a practicing alcoholic. I have not had a drink since.
Let me get right to the point. Even though I quit smoking almost 25 years ago it is killing me. When I die I would imagine that my addiction to cigarettes will be the chief cause of my demise because I have emphysema and asthma, Chronic Obstructive Lung Disease (COPD). Had I not quit smoking when I did I would have been dead long ago. Recently my pulmonologist told me that If I had continued to smoke, I would have needed a lung transplant long ago. For those of you who don’t know me I had a heart transplant in 2007 and smoking may have been a contributor to the heart failure that caused me to need that life-saving surgery.
I know how hard it is to quit smoking and I refuse to accept, “I’ve tried many times and cannot quit.” That, my friend, is pure unadulterated BS. You are only fooling yourself with that nonsense. The fact of the matter is you don’t have the guts to quit. You can’t handle a little discomfort so you light up another smoke and say, “I can’t quit.” And again I say, “BS.” Tough talk? Damned right it is. If you think the discomfort of quitting smoking is hard to handle try the discomfort a of lung cancer as an option, or maybe emphysema.
I smoked up to 4 packs a day for 37 years and I quit. Was it easy? Of course not! It hurt, it was painful, I was an SOB to live with, but damnit I quit. I used every gimmick out there to help me break the habit and finally was rescued by nicotine gum. I probably quit smoking 3 or 4 dozen times maybe more. You see, you don’t quit once, fail and say, “I tried, I can’t quit,” because you haven’t tried. The way to quit smoking is to keep quitting until you quit. You never give up, you quit every day, several times a day until finally you have quit for good.
I always kept my smokes and a lighter in my shirt pocket. Almost every day when I left home for work I would automatically reach for a cigarette and the lighter so I could get my hit of nicotine. Finally, I got to the point where every time I reached into that pocket for the cigarettes and lighter I would pull both out and throw them out the window of the car. I did that every day for weeks. Later in the day I’d find myself buying another pack and a lighter and the next day I would toss them out the window. “The hell with littering,” I would say, “My life’s at stake here.”
After about a year of all this nonsense I finally had my last cigarette in January of 1991. You see, I had just watched my father die of emphysema. At least something good came of his death. I was able to quit. I was addicted to nicotine gum for two years after that and lemon drops for another year but I quit, by God, I quit.
You know why it’s so hard? It is because you are an addict, just like any drunk or junkie. When you hear someone say, “A cigarette tastes so good after a meal,” that’s just more BS. The reason it feels good is because it’s been a while since your last cigarette and you are going into withdrawal. As soon as you light up you stop the withdrawal and feel better. It is no different than getting a hit of heroin or a good slug of booze.
From the time I was 15 years old in 1954 until 1991 (37 years) when I was 52 years old I was a smoker, a heavy smoker. Some days when I went to work I would throw 4 packs of cigarettes in my briefcase and finish them before I retired for the night.. That’s 80 cigarettes.
There are approximately 600 ingredients in cigarettes. When burned, they create more than 7,000 chemicals. At least 69 of these chemicals are known to cause cancer, and many are poisonous as well. Here are just a few of the chemicals in tobacco smoke, and other places they are found:
- Acetone –nail polish remover
- Acetic Acid – ingredient in hair dye
- Ammonia –household cleaner
- Arsenic – rat poison
- Butane – lighter fluid
- Cadmium –battery acid
- Carbon Monoxide car exhaust fumes
- Formaldehyde – embalming fluid
A final note on this subject. In 1998 I lost my wife of 35 years to lung cancer. She, too was a smoker and she died a horrible death, no one should have to suffer the way she did and the way thousands of others do every day. Smoking is a terrible, disgusting and deadly habit. I don’t care who you are, you have a responsibility to yourself and to those who love you to quit smoking. You must. After a while the urges disappear and you can live a normal life again. You might even find that you’ll take great pride in being able to say, “I used to smoke, but I don’t anymore.”
-0-

Feeling better than ever at age 73
Bob Aronson of Bob’s Newheart is a 2007 heart transplant recipient, the founder of Facebook’s over 4,000 member Organ Transplant Initiative (OTI) and the author of most of these donation/transplantation blogs. You may comment in the space provided or email your thoughts to me at bob@baronson.org. And – please spread the word about the immediate need for more organ donors. There is nothing you can do that is of greater importance. If you convince one person to be an organ and tissue donor you may save or positively affect over 60 lives. Some of those lives may be people you know and love. You can register to be a donor at http://www.donatelife.net. It only takes a few minutes.
We Are Too Fat and It’s Killing Us. Obesity — America’s Number One Health Threat.
 By Bob Aronson
By Bob Aronson
Obesity may well be the greatest threat to public health ever, at least that’s the conclusion of a good many national and international health agencies ranging from the American Centers For Disease Control and Prevention (CDC) to the World Health Organization (WHO).
Too many people see obesity as a cosmetic problem and dismiss it as such. It isn’t.  A bad haircut is a cosmetic problem but a bad haircut never killed anyone. Obesity can and does with great regularity. Obesity is not about how you look, it is about slow suicide.
A bad haircut is a cosmetic problem but a bad haircut never killed anyone. Obesity can and does with great regularity. Obesity is not about how you look, it is about slow suicide.
Before we get into the details it is important to define obesity. According to the medical profession men are obese if fat makes up more than 25% of their body weight. Women are obese at more than 30% body fat. In order to measure the percentage of body fat health professionals use a formula called the Body Mass Index (BMI). It is based on height and weight (there is some controversy about the accuracy of BMI in some professional circles but that determination is best made by experts in the field and not by this author. This link will give you more information http://healthland.time.com/2013/08/26/why-bmi-isnt-the-best-measure-for-weight-or-health/
The obesity epidemic is a fact, though, and will continue to be a problem regardless of how the BMI debate is settled).
- A BMI of 18.5 to 24.9 is normal weight.

- 25,0 ti 29.9 is overweight
- 30.0 to 39.9 is obese
- 40.0 and above is extremely obese

You can determine your BMI in private just by clicking on either of the two links below.
- If you want a simple BMI calculator click here. http://www.nhlbi.nih.gov/health/educational/lose_wt/BMI/bmicalc.htm
- If you want a BMI that measures more and is more accurate, click here. http://www.healthstatus.com/calculate/body-fat-percentage-calculator
Studies indicate that nearly one in five US deaths is associated with obesity, which is nearly three times higher than previous estimates. It is now thought that 34% of American adults are obese. Another 34% are overweight.
The preceding information is disturbing enough but even more upsetting is that fact that 17 percent of American children are obese. Another 15% are overweight. That means that a third of our children have weight problems and you can bet that they will carry those problems into adulthood.
So – why worry about all of this, why is it important? It is important because obesity kills. It kills just as sure as a 45 caliber bullet can kill, only it usually takes longer and the death can be painful and far more costly. Bullets are usually mercifully quick. Death by obesity is slower, much slower. It creeps up on you, destroys your organs, debilitates, disables, depresses and costs far more than you can afford and then kills you anyway. It is a long, hard and painful existence, but it can be avoided. It’s not easy, but it can be avoided.
I am writing about obesity because it is a clear and present danger to everyone. According to the National Institutes of Health (NIH) we run the risk of contracting any or all of the following when we ignore warnings about overweight and obesity..
Health Risks of Overweight and Obesity?
http://www.nhlbi.nih.gov/health/health-topics/topics/obe/risks
Being overweight or obese isn’t a cosmetic problem. These conditions greatly raise your risk for other health problems (this list has been edited. To read all of it in detail click on the link above).
Coronary Heart Disease
As your body mass index rises, so does your risk for coronary heart disease (CHD). CHD is a condition in which a waxy substance called plaque (plak) builds up inside the coronary arteries and reduces blood flow to the heart thereby causing a heart attack or heart failure.
High Blood Pressure
Blood pressure is the force of blood pushing against the walls of the arteries as the heart pumps blood. If this pressure rises and stays high over time, it can damage the body in many ways. Your chances of having high blood pressure are greater if you’re overweight or obese.
Stroke
Earlier we talked about a buildup of plaque in your arteries. Well, it can rupture, causing a blood clot to form and if that clot is close to the brain it can cause a stroke. The risk of having a stroke rises as BMI increases.
Type 2 Diabetes
Diabetes is a disease in which the body’s blood sugar, level is too high. In type 2 diabetes, the body’s cells don’t use insulin properly. Diabetes is a leading cause of early death, CHD, stroke, kidney disease, and blindness. Most people who have type 2 diabetes are overweight.
Metabolic Syndrome
Metabolic syndrome is the name for a group of risk factors that raises your risk for heart disease and other health problems, such as diabetes and stroke.
A diagnosis of metabolic syndrome is made if you have at least three of the following risk factors:
- A large waistline. This is called “having an apple shape.” Having extra fat in the waist area is a greater risk factor for CHD than having extra fat in other parts of the body, such as on the hips.
- A higher than normal triglyceride level (or you’re on medicine to treat high triglycerides).
- A lower than normal HDL cholesterol level (or you’re on medicine to treat low HDL cholesterol).
- Higher than normal blood pressure (or you’re on medicine to treat high blood pressure).
- Higher than normal fasting blood sugar (or you’re on medicine to treat diabetes).Being overweight or obese raises your risk for colon, breast, endometrial, and gallbladder cancers.Osteoarthritis is a common joint problem of the knees, hips, and lower back. The condition occurs if the tissue that protects the joints wears away. Extra weight can put more pressure and wear on joints, causing pain or broken bones.Sleep apnea is a common disorder in which you have one or more pauses in breathing or shallow breaths while you sleep.Reproductive Problems
- A person who has sleep apnea may have more fat stored around the neck. This can narrow the airway, making it hard to breathe.
- Sleep Apnea

- Osteoarthritis
- Cancer
- Obesity can cause menstrual issues and infertility in women.

Dementia
- Recent studies show that obesity is linked with brain atrophy. This increases the risk of dementia as people get older.
I think we have pretty well established that obesity can cause irreparable physical harm, but it can cause mental and emotional problems that is just as painful. For example:
- Obesity makes life more difficult. It is harder to tie your shoes, fit in an airplane seat, or find a mate.
- Obese people are stigmatized by society. Many normal weight people look down on obese people.
- Employers discriminate against obese people in hiring, pay increases, and promotions.
- Obesity is a cause of depression in women.
- Obese children rate their quality of life as being even lower than do children who have cancer.
Space does not allow for us to delve farther into adolescent or child obesity but it is a significant problem and we will tackle it in another separate blog.
So now we know about obesity and its effects. Now let’s look into how we get that way and what can be done about it.
The problem and the solution to it seem simple. All you have to do to maintain a healthy weight is to burn up as many calories as you take in. That’s not easy because some people burn calories at a different rate than others. The problem is that few pay any attention to the number or nature of the calories they consume. Furthermore, even fewer people pay any attention to the trade-off of burning them up.
The secret to maintaining a healthy BMI is to be calorie conscious. You should know what you are consuming and how much exercise or activity it takes to burn it off. For example, if you go to a professional football game and eat just one of their hotdogs you will consume about 250 calories. In order to get rid of 250 calories you would need to walk for about an hour (see calorie/exercise  calculator and other calculators here https://www.fitwatch.com If this particular link does not satisfy you just Google calorie calculators and you’ll find dozens of free apps for your phone, tablet, PC or Mac).
calculator and other calculators here https://www.fitwatch.com If this particular link does not satisfy you just Google calorie calculators and you’ll find dozens of free apps for your phone, tablet, PC or Mac).
Obesity does not come on overnight. No one goes to bed fit and in good shape and awakens as a morbidly obese person. The process is gradual and can be stopped at any point along the way if you do two things; 1) Eat right and 2)exercise. That’s all, eat right and exercise.
Most of us live very busy lives and feel as though we don’t have time to cook so “Fast food” becomes a way of life, but there are faster healthy foods that you can prepare for yourself that won’t add inches to your waistline. Try some of these or google “Healthy nutritious and fast food recipes” and you are bound to find something that appeals to you. This site, for example, is very helpful. http://www.eatingwell.com/recipes_menus/collections/quick_healthy_dinner_recipes
Nearly everyone I know has some kind of a sweet tooth. Some have it more than others but almost everyone likes a little “Sweet” now and then and a little might be fine but we just don’t seem to be able to handle just a little. Well, you’d better learn how.
In September 2013, a bombshell report from Credit Suisse’s Research Institute brought into sharp focus the staggering health consequences of sugar on the health of Americans. The group revealed that approximately “30%–40% of healthcare expenditures in the USA go to help address issues that are closely tied to the excess consumption of sugar.” The figures suggest that our national addiction to sugar runs us an incredible $1 trillion in healthcare costs each year. The Credit Suisse report highlighted several health conditions including coronary heart diseases, type II diabetes and metabolic syndrome, which numerous studies have linked to excessive sugar intake.
According to Medicine Net http://www.medicinenet.com/script/main/art.asp?articlekey=56589 Each American consumes one hundred and fifty-six pounds of added sugar. That’s 31 five pound bags of sugar according to the U.S. Department of Agriculture (USDA). Imagine it: 31 five-pound bags for each of us.
In the U.S. diet, the major source of “added sugar” — not including naturally occurring sugars, like the fructose in fruit — is soft drinks. They account for 33% of all added sugars consumed, says Kristine Clark, PhD, RD, a spokeswoman for the Sugar Association. Clark is also director of sports nutrition in the athletic department of Penn State University.
Anne Alexander, editorial director of Prevention and author of The Sugar Smart Diet provided this explanation of what sugars can do to your body.
Glucose
- It seeps through the walls of your small intestine, triggering your pancreas to secrete insulin, a hormone that grabs glucose from your blood and delivers it to your cells to be used as energy.
- But many sweet treats are loaded with so much glucose that it floods your body, lending you a quick and dirty high. Your brain counters by shooting out serotonin, a sleep-regulating hormone. Cue: sugar crash.
- Insulin also blocks production of leptin, the “hunger hormone” that tells your brain that you’re full. The higher your insulin levels, the hungrier you will feel (even if you’ve just eaten a lot). Now in a simulated starvation mode, your brain directs your body to start storing glucose as belly fat.
- Busy-beaver insulin is also surging in your brain, a phenomenon that could eventually lead to Alzheimer’s disease. Out of whack, your brain produces less dopamine, opening the door for cravings and addiction-like neurochemistry.
- Still munching? Your pancreas has pumped out so much insulin that your cells have become resistant to the stuff; all that glucose is left floating in your bloodstream, causing prediabetes or, eventually, full-force diabetes.
Fructose
- It, too, seeps through your small intestine into the bloodstream, which delivers fructose straight to your liver.
- Your liver works to metabolize fructose—i.e., turn it into something your body can use. But the organ is easily overwhelmed, especially if you have a raging sweet tooth. Over time, excess fructose can prompt globules of fat to grow throughout the liver, a process called lipogenesis, the precursor to nonalcoholic fatty liver disease.
- Too much fructose also lowers HDL, or “good” cholesterol, and spurs the production of triglycerides, a type of fat that can migrate from the liver to the arteries, raising your risk for heart attack or stroke.
- Your liver sends an S.O.S. for extra insulin (yep, the multi-tasker also aids liver function). Overwhelmed, your pancreas is now in overdrive, which can result in total-body inflammation that, in turn, puts you at even higher risk for obesity and diabetes Robert Lustig, an endocrinologist from California gained national attention after a lecture he gave titled “Sugar: The Bitter Truth” went viral in 2009. www.youtube.com/watch?v=dBnniua6-oM
Fruit and Sugar substitutes
There are two questions associated with sugar that must be addressed, one has to do with the safety of sugar substitutes and the 2nd with fruit.
Stay away from sugar but eat more fruit! Huh? Fruit is loaded with sugar so how can it possible be good for you? Here is the definitive answer. EAT FRUIT! And here’s why. While fruit does contain sugar it is digested and burned far differently than is the sweetener used in soft drinks, donuts, candy bars and cakes. I could provide you with thousands of words on why fruit is good for you but you don’t need that. What you need to know is this: it is almost impossible to over eat fructose by eating fruit. If you need more details and the research behind the facts click on this link http://well.blogs.nytimes.com/2013/07/31/making-the-case-for-eating-fruit/?_r=0 Fruit can also help keep us from overeating according to Dr. David Ludwig, the director of the New Balance Foundation Obesity Prevention Center at Boston Children’s Hospital. He says, “Unlike processed foods, which are usually digested in the first few feet of our intestines, fiber-rich fruit breaks down more slowly so it travels far longer through the digestive tract, triggering the satiety hormones that tend to cluster further down the small intestines.”
differently than is the sweetener used in soft drinks, donuts, candy bars and cakes. I could provide you with thousands of words on why fruit is good for you but you don’t need that. What you need to know is this: it is almost impossible to over eat fructose by eating fruit. If you need more details and the research behind the facts click on this link http://well.blogs.nytimes.com/2013/07/31/making-the-case-for-eating-fruit/?_r=0 Fruit can also help keep us from overeating according to Dr. David Ludwig, the director of the New Balance Foundation Obesity Prevention Center at Boston Children’s Hospital. He says, “Unlike processed foods, which are usually digested in the first few feet of our intestines, fiber-rich fruit breaks down more slowly so it travels far longer through the digestive tract, triggering the satiety hormones that tend to cluster further down the small intestines.”
That brings us to the issue of artificial sweeteners. There’s still a lot we don’t know about them and research is still being done but the scientific community generally believes that they are not harmful. T hey urge caution, though, and say that if you must have something sweet, go with the artificial variety preferably Stevia. But, the jury is still out and its best to avoid all sweeteners if possible. You can find more details in the report from CNN’s Dr. Sanjay Gupta. http://www.everydayhealth.com/sanjay-gupta/myths-and-facts-about-sugar-substitutes.aspx
hey urge caution, though, and say that if you must have something sweet, go with the artificial variety preferably Stevia. But, the jury is still out and its best to avoid all sweeteners if possible. You can find more details in the report from CNN’s Dr. Sanjay Gupta. http://www.everydayhealth.com/sanjay-gupta/myths-and-facts-about-sugar-substitutes.aspx
While there’s no medical evidence these sugar substitutes are dangerous, a recent study suggests they don’t guarantee weight loss either. Researchers from the Yale University School of Medicine found that eating foods with artificial sweeteners when we’re hungry or tired increases the likelihood of choosing higher-calorie foods later on.
“We still don’t fully understand the long-term effects of artificial sweeteners,” says Alexandra Kaplan Corwin, a registered dietician in the division of pediatric endocrinology and diabetes at The Children’s Hospital at Montefiore Medical Center in New York City. “Though the [U.S. Food and Drug Administration] has said they’re safe and the National Cancer Institute says they don’t cause cancer, we still don’t really know if there are long-term health consequences.”
Conclusion
We’ve discussed obesity, it’s causes, the dangers of sugar and the advantages of eating more fruit. Now the ultimate question, if you are obese, how do you lose that excess weight? Most experts will tell you that almost any program will help you lose weight. The real trick, though, is losing it and keeping it off. It would be quite easy to list a number of diets and let you choose, but that would not be helpful because everyone’s condition is different. We suggest that your very first step is to talk to your primary care physicians about the options he or she believes best suit you. Your physician knows your medical history and is far better able to make wise recommendations that the writer of a blog. What I can say without fear of contradiction is that before you take on any weight loss program you must first assess your total medical condition. If you do not you could be headed for trouble. Your doctor will either make diet recommendations or direct you to someone who can.
Chances are that if you read this blog you are have more than a passing acquaintance with the Internet and will continue to do some research on your own on how to get rid of those excess pounds. Well, we anticipated that and found one link in particular that might offer significant help. http://www.cdc.gov/healthyweight/index.html Clicking here will lead you to scores of sites that can help you achieve the weight loss goals you seek.
-0-
Feeling better than ever at age 76
Bob Aronson of Bob’s Newheart is a 2007 heart transplant recipient, the founder of Facebook’s over 4,000 member Organ Transplant Initiative (OTI) and the author of most of these donation/transplantation blogs. You may comment in the space provided or email your thoughts to me at bob@baronson.org. And – please spread the word about the immediate need for more organ donors. There is nothing you can do that is of greater importance. If you convince one person to be an organ and tissue donor you may save or positively affect over 60 lives. Some of those lives may be people you know and love. You can register to be a donor at http://www.donatelife.net. It only takes a few minutes.
Bob’s NewHeart — The Impossible Dream
As the group I founded, Facebook’s Organ Transplant Initiative (OTI) grows so do the number of questions that we get. There are so many people who are deathly ill and waiting for organ transplants and they all have a multitude of questions. That waiting period can be frightening because because patients really are forced to face their mortality.
My heart transplant was almost 8 years ago so while not an expert I have some experience that might interest both pre and post transplant patients.
Those awaiting organs want to know about “The call” how long I was on the list and whether recovery from the surgery was difficult.
Those who are new recipients are always interested in what lies ahead. I’m hoping this blog answers some of those questions.
Every transplant patient is different, our bodies, minds and conditions are different. My story speaks to my situation. I hope it helps others have a better understanding of what it’s like to be told you are dying and how it feels to get the “Gift of life.”
I wrote the following blog about two years ago. It is my story. I’d like to hear yours and would also appreciate any comments you choose to make.

“Some men see things as they are and say why.
I dream things that never were and say, why not”
George Bernard Shaw
This is post number 200 in the Bob’s Newheart Series of blogs on organ donation/transplantation and related issues
On February 17, 2014 I will turn 75. It is an incredible feat for someone who abused his body as badly as I did. By my count I have been dead three times. Once from sudden cardiac arrest, once during surgery in a hospital and I suppose once when they took my heart out to give me a new one (maybe that one doesn’t count). I have to believe that I am only alive today because I was given a mission to do everything in my power to help others who face critical and/or life threatening illnesses. The social media offer me that opportunity and I have gladly…
View original post 8,480 more words
How To Live Healthy, Live Long and Stay off the Transplant List
By Bob Aronson

As of today here is the latest data from the United Network For Organ Sharing (UNOS). There are 123,961 people on the U.S. transplant waiting list; from January through August of this year there have been 19,426 transplanted organs from 9,512 donors. Do the math and you will find that most of those nearly 127,000 will NOT get organs anytime soon. Many, nearly 7,000 will die waiting. Why? The answer is simple, only about 40% of Americans become donors even though almost everyone agrees that donation is a good idea. The fact is, most of us just don’t get around to signing up. We have been putting it off since the Transplant Act was passed in 1984. Anyone who thinks donation alone will end the shortage is fooling themselves. It won’t…EVER! Sure we have to keep encouraging people to donate…we can’t let up but we have to consider alternatives. We must!
The key to solving the shortage of transplantable organs is to significantly diminish the demand.
“We have met the enemy and he is us,” has become a trite expression bu1ht that doesn’t make it any less true. We are our own worst enemies. The numbers are staggering. We are killing ourselves in four ways:
- We drink too much alcohol
- We smoke too much
- We eat too much of the wrong food
- We don’t get anywhere near enough exercise
Let’s look at he facts:
 Alcohol abuse. 5% of Americans abuse alcohol or are alcohol dependent, The estimated annual medical expenditures associated with alcohol abuse total $26.3 billion. Organs most commonly affected are the lungs, kidneys, pancreas, heart and liver.
Alcohol abuse. 5% of Americans abuse alcohol or are alcohol dependent, The estimated annual medical expenditures associated with alcohol abuse total $26.3 billion. Organs most commonly affected are the lungs, kidneys, pancreas, heart and liver.

- 22.5% of Americans are current smokers, resulting in significant health problems
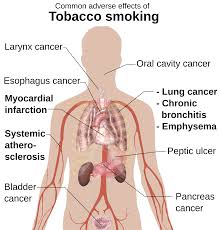 and associated costs. Medical costs caused by cigarette smoking exceed $75 billion a year. According to the Centers for Disease Control in Atlanta, Georgia, Smoking harms nearly every organ of the body and causes many diseases. Cigarette smoking remains the single most-common preventable cause of death in the United States. The adverse health effects from cigarette smoking account for more than 440,000 deaths, or nearly one of every five deaths, each year in the United States.
and associated costs. Medical costs caused by cigarette smoking exceed $75 billion a year. According to the Centers for Disease Control in Atlanta, Georgia, Smoking harms nearly every organ of the body and causes many diseases. Cigarette smoking remains the single most-common preventable cause of death in the United States. The adverse health effects from cigarette smoking account for more than 440,000 deaths, or nearly one of every five deaths, each year in the United States.

 About 40 plus % of adults in the United States are obese. Often caused by eating too much of the wrong food, a good number of obese people experience some organ failure. The direct medical costs for obesity have been approximated at $51.6 billion per year. The organs most often affected are the heart, kidneys and pacnreas.
About 40 plus % of adults in the United States are obese. Often caused by eating too much of the wrong food, a good number of obese people experience some organ failure. The direct medical costs for obesity have been approximated at $51.6 billion per year. The organs most often affected are the heart, kidneys and pacnreas.

- Lack of Exercise. A study released by the Centers For Disease Control (CDC) estimates
 that nearly 80 percent of adult Americans do not get the recommended amounts of exercise each week, potentially setting themselves up for years of health problems. Physical inactivity can lead to obesity and Type 2 diabetes, according to the CDC, while exercise can help control weight, and reduce the risk for developing heart disease and some cancers, while providing mental health benefits.
that nearly 80 percent of adult Americans do not get the recommended amounts of exercise each week, potentially setting themselves up for years of health problems. Physical inactivity can lead to obesity and Type 2 diabetes, according to the CDC, while exercise can help control weight, and reduce the risk for developing heart disease and some cancers, while providing mental health benefits.

This blog is about meeting the organ shortage by preventing organ failure. One way to do that is to lead healthier lifestyles. Alcohol abuse and tobacco use are obvious culprits and we won’t go into detail here. You should know to severely limit alcohol and quit using tobacco altogether and if not just Google the topics, there are thousands of resources. So, let’s concentrate on food and exercise. Let’s start with food. There are two lists here, 1) the worst foods and 2) the best foods.
Top 30 Worst Foods in America (from Food Matters
Note from Bob’s Newheart. While Food Matters lists 30 I am only listing ten. You can click on their link for the rest of the story)
Today’s food marketers have loaded many of their offerings with so much fat, sugar, and sodium that eating any of the foods in this article on a daily basis could destroy all your hard work and best intentions of eating healthy. This list is brought to you by Eat This Not That and Men’s Health. http://foodmatters.tv/articles-1/the-30-worst-foods-in-america-beware
- Worst Meal in America
 Carl’s Jr. Six Dollar Guacamole Bacon Burger with Medium Natural Cut Fries and 32-oz Coke 1,810 calories – 92 g fat (29.5 g saturated, 2 g trans) – 3,450 mg sodium
Carl’s Jr. Six Dollar Guacamole Bacon Burger with Medium Natural Cut Fries and 32-oz Coke 1,810 calories – 92 g fat (29.5 g saturated, 2 g trans) – 3,450 mg sodium
Of all the gut-growing, heart-threatening, life-shortening burgers in the drive-thru world, there is none whose damage to your general well-being is as potentially catastrophic as this. A bit of perspective is in order: This meal has the caloric equivalent of 9 Krispy Kreme Original Glazed doughnuts, the saturated fat equivalent of 30 strips of bacon, and the salt equivalent of 10 large orders of McDonald’s French fries!
- Worst Drink
Baskin-Robbins Large Chocolate Oreo Shake. 2,600 calories – 135 g fat (59 g saturated, 2.5 g trans) – 1,700 mg sodium – 263 g sugars. We didn’t think anything could be worse than Baskin-Robbins’ 2008 bombshell, the Heath Bar Shake. After all, it had more sugar (266 grams) than 20 bowls of Froot Loops, more calories (2,310) than 11 actual Heath Bars, and more ingredients (73) than you’ll find in most chemistry sets. Yet the folks at Baskin-Robbins have shown that when it comes to making America fat, they’re always up to the challenge. The large Chocolate Oreo Shake is soiled with more than a day’s worth of calories and 3 days’ worth of saturated fat. Worst of all, it takes less than 10 minutes to sip through a straw.
- Worst Ribs
Outback Steakhouse Baby Back Ribs 2,580 calories. Let’s be honest: Ribs are rarely served alone on a plate. When you add a sweet potato and Outback’s Classic Wedge Salad, this meal is a 3,460-calorie blowout. (Consider that it takes only 3,500 calories to add a pound of fat to your body. Better plan for a very, very long “walkabout” when this meal is over!)
4.Worst Pizza
Uno Chicago Grill Classic Deep Dish Individual Pizza. 2,310 calories – 165 g fat (54 g saturated) – 4,920 mg sodium – 120 g carbs.  The problem with deep dish pizza (which Uno’s knows a thing or two about, since they invented it back in 1943) is not just the extra empty calories and carbs from the crust, it’s that the thick doughy base provides the structural integrity to house extra heaps of cheese, sauce, and greasy toppings. The result is an individual pizza with more calories than you should eat in a day and more sodium than you would find in 27 small bags of Lays Potato Chips. Oh, did we mention it has nearly 3 days’ worth of saturated fat, too? The key to success at Uno’s lies in their flatbread pizza.
The problem with deep dish pizza (which Uno’s knows a thing or two about, since they invented it back in 1943) is not just the extra empty calories and carbs from the crust, it’s that the thick doughy base provides the structural integrity to house extra heaps of cheese, sauce, and greasy toppings. The result is an individual pizza with more calories than you should eat in a day and more sodium than you would find in 27 small bags of Lays Potato Chips. Oh, did we mention it has nearly 3 days’ worth of saturated fat, too? The key to success at Uno’s lies in their flatbread pizza.
- Worst Mexican Dish
Chili’s Fajita Quesadillas Beef with Rice and Beans, 4 Flour Tortillas, and Condiments. 2,240 calories – 92 g fat (43.5 g saturated) – 6,390 mg sodium – 253 g carbs. Since when has it ever been a smart idea to combine 2 already calorie- and sodium-packed dishes into one monstrous meal? This confounding creation delivers nearly a dozen Krispy Kreme original glazed doughnuts worth of calories, the sodium equivalent of 194 saltine crackers, and the saturated fat equivalent of 44 strips of bacon. Check please.
- Worst Seafood Dish
Romano’s Macaroni Grill Parmesan Crusted Sole. 2,190 calories – 141 g fat (58 g saturated) – 2,980 mg sodium – 145 g carbs. Fish is normally a safe bet, but this entrée proves that it’s all in the preparation. If you fry said fish in a shell of cheese, be prepared to pay the consequences. Here that means meeting your daily calorie, fat, saturated fat, and sodium intake in one sitting.
- Worst Chinese Dish
 P.F. Chang’s Combo Lo Mein. 1,968 calories – 96 g fat (12 g saturated) – 5,860 mg sodium. Lo mein is normally looked at as a side dish, a harmless pile of noodles to pad your plate of orange chicken or broccoli beef. This heaping portion (to be fair, Chang’s does suggest diners share an order) comes spiked with chicken, shrimp, beef, and pork, not to mention an Exxon Valdez-size slick of oil. The damage? A day’s worth of calories, 1 ½ days’ worth of fat, and 2 ½ days’ worth of sodium. No meat-based dish beats out the strip.
P.F. Chang’s Combo Lo Mein. 1,968 calories – 96 g fat (12 g saturated) – 5,860 mg sodium. Lo mein is normally looked at as a side dish, a harmless pile of noodles to pad your plate of orange chicken or broccoli beef. This heaping portion (to be fair, Chang’s does suggest diners share an order) comes spiked with chicken, shrimp, beef, and pork, not to mention an Exxon Valdez-size slick of oil. The damage? A day’s worth of calories, 1 ½ days’ worth of fat, and 2 ½ days’ worth of sodium. No meat-based dish beats out the strip.
- Worst Appetizer
On the Border Firecracker Stuffed Jalapenos with Chili con Queso. 1,950 calories – 134 g fat (36 g saturated) – 6,540 mg sodium. Appetizers are the most problematic area of most chain-restaurant menus. That’s because they’re disproportionately reliant on the type of cheesy, greasy ingredients that catch hungry diners’ eyes when they’re most vulnerable—right when they sit down. Seek out lean protein options like grilled shrimp skewers or ahi tuna when available; if not, simple is best—like chips and salsa.
- Worst Burger
Chili’s Smokehouse Bacon Triple Cheese Big Mouth Burger with Jalapeno Ranch Dressing. 1,901 calories – 138 g fat (47 g saturated) – 4,201 mg sodium. Any burger whose name is 21 syllables long is bound to spell trouble for your waistline. This burger packs almost an entire day’s worth of calories and 2 ½ days’ worth of fat. Chili’s burger menu rivals Ruby Tuesday’s for the worst in America, so you’re better off with one of their reasonable Fajita Pitas to silence your hunger.
10. Worst Sandwich
Quizno’s Large Tuna Melt 1,760 calories – 133 g fat (26 g saturated, 1.5 g trans) – 2,120 mg sodium. In almost all other forms, tuna is a nutritional superstar, so how did it end up as the headliner for America’s Worst Sandwich? Blame an absurdly heavy hand with the mayo the tuna is mixed with, along with Quiznos’ larger-than-life portion sizes. Even though they’ve managed to trim this melt down from the original 2,000-plus calorie mark when we first tested it, it still sits squarely at the bottom of the sandwich ladder.
nutritional superstar, so how did it end up as the headliner for America’s Worst Sandwich? Blame an absurdly heavy hand with the mayo the tuna is mixed with, along with Quiznos’ larger-than-life portion sizes. Even though they’ve managed to trim this melt down from the original 2,000-plus calorie mark when we first tested it, it still sits squarely at the bottom of the sandwich ladder.
Now you know what to avoid, and we urge you to click on the Food Matters link to read the whole list. So, if you can’t eat any of the aforementioned items what do you eat? There’s plenty to choose from. Health Life lists 100 and you can read them all by clicking on their link. Here are their top ten.
http://www.dwlz.com/HealthyLife/healthy50.html
| THE 100 HEALTHIEST FOODS | ||
| Fruit | Fat/Calorie Breakdown | Body Benefits |
( 1) Apples 1) Apples |
1 medium apple: 81 calories, 0 g fat |
An apple’s 3 g of fiber help you meet your fiber goal of 20 g to 30 g daily. High-fiber diets can lower heart disease risk. |
| (2) Apricots | 3 apricots: 51 calories, 0 g fat |
A good source of beta-carotene (which is converted to vitamin A by the body), providing the equivalent of 35% of the RDA for vitamin A |
| (3) Bananas | 1 medium: 105 calories, 0 g fat |
Bananas are a great source of potassium, which plays a key role in heart health and muscle function. Plus each one has 2 g of fiber. |
| (4) Blackberries | 1 cup: 74 calories, 0 g fat |
This fruit boasts a whopping 10 g of fiber in a single cup. |
| (5) Blueberries | 1 cup: 81 calories, 0 g fat |
Blueberries help prevent and treat bladder infections by making it hard for bacteria to stick to urinary tract walls. |
| (6) Cantaloupe | 1 cup, cubed: 84 calories, 1 g fat |
An antioxidant double whammy, with 68 mg of vitamin C and enough beta-carotene to cover 65% of your daily vitamin A quota. |
| (7) Cherries | 1 cup: 84 calories, 1 g fat |
A good source of perillyl alcohol, which helps prevent cancer in animals. Heart-protective anthocyanins give cherries their color. |
| (8) Cranberry juice |
1 cup: 144 calories, 0 g fat |
Fights bladder infections the same way blueberries do. |
| (9) Grapefruits | 1/2 fruit: 39 calories, 0 g fat |
A good source of vitamin C and a compound called naringenin, which helps suppress tumors in animals. |
| (10) Purple grapes and juice |
1 cup seedless: 113 calories, 9 g fat |
Offer three heart-guarding compounds: flavonoids, anthocyanins and resveratrol. (Green grapes are not rich in them) |
If you insist on eating meat there are some good choices you can make…we’ll jump ahead on the list to give you a sneak preview.
| Beef | 3 oz, cooked: 150 to 280 calories, 5 g to 20 g fat |
Beef is a good source of both CLA and iron, but since it’s also high in saturated fat, have it no more than three times a week. |
| Chicken, without skin |
3 oz, cooked: 162 calories, 6 g fat |
Remove the skin and you’ve got an excellent, low fat source of protein. And 3 oz provides 38% of the RDA for the B vitamin niacin. |
| ( Lamb | 3 oz, cooked, trimmed of fat: 175 calories, 8 g fat |
Lamb, like beef, is also a good source of CLA. Ditto beef’s saturated fat warning and wee kly consumption recommendation. kly consumption recommendation. |
| Lean pork |
3 oz, cooked, trimmed of fat: 140 calories, 4 g fat |
Fat-trimmed pork tenderloin has one-third less fat than even lean beef. And it boasts 71% of the RDA for thiamine. |
If Healthy Life doesn’t offer you enough good food ideas, here are some other excellent resources for you to peruse.
Exercise
Ok, now lets talk exercise. Why is it important and what should you be doing to stay fit and healthy. For more on that subject we turn to the famed Mayo Clinic. Here’s what they say:
 How much should the average adult exercise every day? http://www.mayoclinic.org/healthy-living/fitness/expert-answers/exercise/faq-20057916
How much should the average adult exercise every day? http://www.mayoclinic.org/healthy-living/fitness/expert-answers/exercise/faq-20057916
- Aerobic activity.Get at least 150 minutes a week of moderate aerobic activity or 75 minutes a week of vigorous aerobic activity. You also can do a combination of moderate and vigorous activity. The guidelines suggest that you spread out this exercise during the course of a week.
- Strength training.Do strength training exercises at least twice a week. No specific amount of time for each strength training session is included in the guidelines.
Moderate aerobic exercise includes such activities as brisk walking, swimming and mowing the lawn. Vigorous aerobic exercise includes such activities as running and aerobic dancing. Strength training can include use of weight machines or activities such as rock climbing or heavy gardening.
As a general goal, aim for at least 30 minutes of physical activity every day. If you want to lose weight or meet specific fitness goals, you may need to exercise more. Want to aim even higher? You can achieve more health benefits, including increased weight loss, if you ramp up your exercise to 300 minutes a week.
Short on long chunks of time? Even brief bouts of activity offer benefits. For instance, if you can’t fit in one 30-minute walk,  try three 10-minute walks instead. What’s most important is making regular physical activity part of your lifestyle.
try three 10-minute walks instead. What’s most important is making regular physical activity part of your lifestyle.
Other exercise links:
http://www.nhs.uk/Livewell/fitness/Pages/physical-activity-guidelines-for-adults.aspx
-0-
A message from Bob Aronson, Founder of Bob’s Newheart blogs.
 Bob’s Newheart was established to support and help everyone, but particularly those who need or have had organ transplants. Most of our blogs specifically address donation/transplantation issues while others are more general, but they are all related. Because anti-rejection drugs compromise immune systems, transplant recipients are more susceptible to a variety of diseases. We provide general health and medical information to help them protect themselves while at the same time, helping others live healthier lives and avoid organ failure.
Bob’s Newheart was established to support and help everyone, but particularly those who need or have had organ transplants. Most of our blogs specifically address donation/transplantation issues while others are more general, but they are all related. Because anti-rejection drugs compromise immune systems, transplant recipients are more susceptible to a variety of diseases. We provide general health and medical information to help them protect themselves while at the same time, helping others live healthier lives and avoid organ failure.
The Bob’s Newheart mission is three-fold; 1) to provide news and information that promotes healthier living so people won’t need transplants; 2) To help recipients protect their new organs and; 3) to do what we can to ensure that anyone who needs an organ can get one. About 7,000 Americans die every year while waiting for a life-saving organ. I am sure you will agree that should not happen.
In the U.S. the great majority of people support organ donation, but only about 40% of us officially become organ donors. Many have good intentions but just don’t get around to it.
No one likes thinking about their ultimate demise, but we all know there’s no way of predicting how long we will live. There are just too many intangibles. My transplanted heart came from a 30 year old man. I’m sure he had no intention of being a donor at that age. So why leave donation to chance? If you are not yet a donor, please register at www.donatelife.net it only takes a few seconds. Then, tell your family about your decision so there is no confusion when the time comes to donate.
One organ donor can save or positively affect the lives of up to 60 people. There is no nobler thing you can do than becoming an organ donor.
A Better Way to Combat Obesity
By Dr. Priscilla Diffie-Couch
Introduction by Bob Aronson
Obesity is an equal opportunity disease. It is no respecter of age, gender, race or religion. It is deadly and growing so that it now affects more than a third of U.S. adults (nearly 80 million people). According to the Obesity Society, 69 percent of American adults are either affected by obesity or having excess weight. http://www.obesity.org/resources-for/what-is-obesity.htm
The National Institutes of Health (NIH) says the combination of poor diet and physical inactivity cause about 300.000 deaths a year, the second leading cause of preventable death in the U.S.
Obesity puts individuals at risk for more than 30 chronic health conditions including: type 2 diabetes, high cholesterol, hypertension, gallstones, heart failure, fatty liver disease, sleep apnea, GERD, stress incontinence, heart failure, degenerative joint disease, birth defects, miscarriages, asthma, and numerous cancers.
Priscilla Diffie-Couch E.E.D. has been researching and writing about health issues for over two decades. Her reporting is factual, objective, helpful and frank. She is a frequent contributor to Bob’s Newheart.
A Better Way to Combat Obesity
By Priscilla Diffie-Couch E.E.D

Obesity is more than an abundance of food and a shortage of exercise. It is more than the substitution of sugar for fat or the easy access to cheap fast foods. Few would question the ever-increasing obsession with food or need to get to the root of that problem. But too few treat obesity as a genuine threat. Yet what good does it do to make the world safe from terrorism while we watch millions of people being held hostage by food until they eat themselves to death?
 What caused Americans to get so fat? Research is replete with the absolute proof that eating fat does not cause us to get fat ( www.wnyc.org/story/eating–fat–doesnt–make–us–fat). In fact, we have learned that the introduction of low-fat food into our diet was one of the greatest health mistakes ever made. We have only learned lately that, with the exception of transfat, fat is not a culprit in causing disease. On the contrary, when we remove fat from our diet, we deprive ourselves of vital nutrients that prevent disease, in particular, vitamin D ( medicinenet.com/ vitamin_d_deficiency/related…/index.htm ).
What caused Americans to get so fat? Research is replete with the absolute proof that eating fat does not cause us to get fat ( www.wnyc.org/story/eating–fat–doesnt–make–us–fat). In fact, we have learned that the introduction of low-fat food into our diet was one of the greatest health mistakes ever made. We have only learned lately that, with the exception of transfat, fat is not a culprit in causing disease. On the contrary, when we remove fat from our diet, we deprive ourselves of vital nutrients that prevent disease, in particular, vitamin D ( medicinenet.com/ vitamin_d_deficiency/related…/index.htm ).
A shocking number of diseases are associated with low levels of vitamin D: Alzheimer’s, dementia, diabetes, fatty liver, high blood pressure, Chron’s disease, allergy, MS, depression, osteopenia, cancer, rickets, cystic fibrosis, celiac disease and obesity itself. Reliable recent evidence shows that many Americans are short of vitamin D (health.usnews.com/…/many-americans-fall-short-on-their-vitamin–d).
Making matters worse, obese people do not make as much vitamin D3 in their guts as normal weight people do. That exacerbates the shortage of vitamin D. In one study obese subjects had significantly lower basal 25-hydroxyvitamin D concentrations and higher parathyroid hormone concentrations than did age-matched control subjects. Evaluation of blood vitamin D3 concentrations 24 hours after whole-body irradiation showed that the incremental increase in vitamin D3 was 57% lower in obese than in non-obese subjects (ajcn.nutrition.org/content/72/3/690.abstract).
Besides the fact that low levels of vitamin D contribute to obesity and obesity further reduces levels of vitamin D, we are caught in another vicious cycle. Omitting fat deprives us of the unequalled satiating power of full-fat foods. That circles us right back into further weight gain.
Another result compounds the problem. Food without fat loses much of its flavor. So food manufacturers fill that void with added sugar and
 salt. But neither the presence of sugar or salt is independently responsible for the fattening of America. Our bodies have always been able to tolerate salt and sugar in controlled amounts. It is the unregulated unparalleled quantities of sugar in our foods–not ingested fat–that turns to fat in the human body.
salt. But neither the presence of sugar or salt is independently responsible for the fattening of America. Our bodies have always been able to tolerate salt and sugar in controlled amounts. It is the unregulated unparalleled quantities of sugar in our foods–not ingested fat–that turns to fat in the human body.
Upon closer observation, it is not just the quantity of sugar that causes our bodies to lose essential metabolic control. It turns out that simple carbohydrates in any food form are treated the same as sugar when we ingest them. Table sugar and white bread work equally efficiently to impair our body’s ability to use insulin. And that causes constant hunger and disease and bulging bodies. Bulging bodies crave food.
So someone came up with the brilliant idea of replacing sugar in food and drink. Along came the introduction of sugar substitutes, possibly the second biggest health mistake ever made. Recent research strongly suggests that sweeteners cause blood sugar spikes. (See the study published in Nature, September 17, 2014 “Artificial Sweeteners Induce Glucose Intolerance by Altering Gut Bacteria.”) The negative consequences are the same–possibly worse. Drinks sweetened with sugar substitutes have zero calories. So we happily consume greater quantities of sugar-free food and drink with abandon, never realizing how much this contributes to our weight problem.
That still does not fully explain why we are getting more and more obese as a nation. Obviously, easy access to abundant food and drink of any  kind makes it harder to control our weight. The super-sizing of everything we eat is now so common that we feel cheated if we are offered what once was a normal sized hamburger or portion of fries. The original six ounce soda now seems like a drink intended for a small child. Just as we have readjusted our view of what is overweight because there are so many more overweight people than ever before, we have readjusted our view of portion size. That results in eating far more calories than ever before.Is quantity then the real culprit in packing on the pounds? Without a doubt, it is a major contributor to obesity. A summary reported in April of this year by Whole Health Source charts the rise in calorie intake and its impact on obesity. “Calorie Intake and the U.S. Obesity Epidemic” points out that Americans increased their total calorie intake by 363 calories a day between 1960 and 2009. Surprisingly, during this time obesity has trebled yet we have cut our intake of fat from 45% of total calorie to less than 33%. What is not so surprising is that we now consume mostly simple carbohydrates. (www.hsph.harvard.educ/nutritionsource/fats-full-story/).
kind makes it harder to control our weight. The super-sizing of everything we eat is now so common that we feel cheated if we are offered what once was a normal sized hamburger or portion of fries. The original six ounce soda now seems like a drink intended for a small child. Just as we have readjusted our view of what is overweight because there are so many more overweight people than ever before, we have readjusted our view of portion size. That results in eating far more calories than ever before.Is quantity then the real culprit in packing on the pounds? Without a doubt, it is a major contributor to obesity. A summary reported in April of this year by Whole Health Source charts the rise in calorie intake and its impact on obesity. “Calorie Intake and the U.S. Obesity Epidemic” points out that Americans increased their total calorie intake by 363 calories a day between 1960 and 2009. Surprisingly, during this time obesity has trebled yet we have cut our intake of fat from 45% of total calorie to less than 33%. What is not so surprising is that we now consume mostly simple carbohydrates. (www.hsph.harvard.educ/nutritionsource/fats-full-story/).
Substituting simple for complex carbohydrates changes the food equation. What is almost always missing when we eat the wrong foods in any quantity is fiber. Fiber is a magic agent that prevents sweetened food and drink from causing a sharp insulin spike (www.sharecare.com/health/type-2…/food-and-blood-sugar–levels). Fiber is the friendly element in food that causes us to detect texture and tricks our stomachs into feeling fuller on less quantity. We need from 25 to 35 grams of fiber daily. Yet it impossible to find a single meal when we eat out that offers more than two or three grams of fiber, if that. Even when we eat at home, we fill our plates with everything but fiber.
always missing when we eat the wrong foods in any quantity is fiber. Fiber is a magic agent that prevents sweetened food and drink from causing a sharp insulin spike (www.sharecare.com/health/type-2…/food-and-blood-sugar–levels). Fiber is the friendly element in food that causes us to detect texture and tricks our stomachs into feeling fuller on less quantity. We need from 25 to 35 grams of fiber daily. Yet it impossible to find a single meal when we eat out that offers more than two or three grams of fiber, if that. Even when we eat at home, we fill our plates with everything but fiber.
Eating to stay slim requires daily monitoring of what we put in our bodies. It is not easy. Yet, Americans have continued to search for some simple formula for fighting the fat that creeps on to our bodies more readily with each passing year. Diet pills don’t work. Diet plans are a dismal failure.
It goes without saying that Americans are less active now than ever before in history. The sad fact is that, the  fatter people are, the harder it is to be active. Slim people tell fat people to walk. They can’t. Many rely on riding on special carts to even be able to navigate through the grocery store. The amount of effort required to lose only a few pounds causes too many of the overweight and obese simply to give up.
fatter people are, the harder it is to be active. Slim people tell fat people to walk. They can’t. Many rely on riding on special carts to even be able to navigate through the grocery store. The amount of effort required to lose only a few pounds causes too many of the overweight and obese simply to give up.
So what is the solution to obesity? No one seems to know. Individually, however, I feel certain that we could make a discernible dent in the problem by doing something very simple. Retrain ourselves and our children to abide by the nutrition rules that worked so well back when obesity was a rare burden. Every meal should consist of single portions on a 10-inch dinner plate (except for salad) consisting of 30% full fat, 30% protein, and 60% complex carbohydrates, which contain multiple grams of fiber. Substantial gains in loss of fatness could be achieved if we asked ourselves before every meal or snack, “Where is the fiber?”
Allowing ourselves and our children dessert only if we followed the rules for healthy eating spelled out above would provide a bonus for maintaining a healthy weight.
But most of us know what we should do individually to avoid getting fat. Having that knowledge has yet to solve the obesity problem. We have been left alone too long. Sporadic solutions are not the answer. Companies that have independently created incentive programs that reward people who lose weight find themselves subject to discrimination lawsuits.
I cringe as I write these words but I have come to believe that we have no choice but to get the government of every nation with an obesity problem directly involved. Independent drug researchers are never going to discover the magic fat-dissolving pill. National research agencies must be fully funded to seek causes and solutions for the world-wide obesity malady. New standards for defining obesity must be based on actual medical outcomes. Validity of using Body Mass Index or waist circumference for predicting negative health effects must be re-examined and adjusted for age. Meanwhile, steps need to be taken to implement workable plans to gain a foothold in arresting obesity. I have never been an advocate of total government intervention. But, when every possible private option has been exhausted, imposing universal programs may be the only answer.
The government must step up to reduce the burden of being fat. There are at least 300,000 reasons why. That is the number of deaths per year in the US estimated to be associated with obesity. More than 78 million Americans can now be classified as obese. That is more than the combined populations of California, Texas and New York. If the current trend continues, by 2030 that number will increase to a shocking 45 to 51% of the population.
Obesity is now the second leading preventable cause of death in our country. It is linked to sixty chronic conditions like diabetes, high blood pressure, stroke, heart disease, osteoporosis, breast cancer and others. It is now safer to smoke, drink to excess, or be impoverished than it is to be obese.
chronic conditions like diabetes, high blood pressure, stroke, heart disease, osteoporosis, breast cancer and others. It is now safer to smoke, drink to excess, or be impoverished than it is to be obese.
The fatter we get, the less active we are. The less active we are, the sicker we get. The sicker we get, the greater the demand for costly drugs and hospital care and doctor visits. The more we spend on medical care, the more stress we feel. The more stress we feel, the more we turn to food. Clearly, the problem of obesity has ballooned into a never-ending cycle.
This cycle is not easily broken. Sadly, in a routine trip to the grocery store, we can see a disturbing number of people so obese that they could have been found only in “freak” shows fifty years ago. We are no longer surprised to see a rack of size 5X clothing on display at Wal-Mart. Ironically, the fatter we get, the fewer of us see ourselves as fat. By current definition, an ordinary person six foot tall who weighs 221 pounds is classified as obese. But because one in three Americans is now overweight, our perception of “fatness” has changed. Fat people look at fatter people with disgust. Other people are fat. We just need to lose a few pounds.
Losing pounds is not easy. Studies show that most of us underestimate our calorie intake and overestimate our level of activity. Fat people sit on the sidelines while others ride bikes, hit  tennis balls and swim. Fat kids watch TV and sit in front of computers while their slimmer counterparts run and play. The multi-billion dollar diet industry has failed. The misguided low-fat diet craze has failed. The only success story we can point to is the supersizing of America.
tennis balls and swim. Fat kids watch TV and sit in front of computers while their slimmer counterparts run and play. The multi-billion dollar diet industry has failed. The misguided low-fat diet craze has failed. The only success story we can point to is the supersizing of America.
What will it take to break this supersizing cycle? Thirteen years later, we are still aware of the changes in our lives prompted by the attack on 9-11-2001. If terrorists had killed 300,000 Americans that day—as obesity does each year–it is hard to imagine the extent of government intervention in our lives aimed at protecting our safety and well-being.
What will it take to wake us up? Obesity now claims more lives than illicit drug use, car and plane wrecks combined. In 2009 alone, obesity cost our nation $152 billion. These enormous costs are borne by us all. They show no signs of abating. Individual efforts to curb obesity have failed. That leaves little choice but to turn to the government for solutions.
The specific role of government should take the form of incentives, not mandates like those used in national security. Medical research needs to be funded to provide clear guidance for designing programs that can break the cycle of disease and disorders resulting from being fat. Government must first focus on finding out why we are fat and then on prevention. Providing specific incentives associated with being fit not fat must be incorporated into the infrastructure of our lives. A massive campaign must be mounted to make the public aware of these new programs.
Such government programs should begin early in our public schools. Required physical education classes should be reinstated from primary through the twelfth grade. Physical fitness should be given prestigious treatment among honors awarded to students of all ages. Teachers in every field of study should be rewarded for creating curricula that require students to get up move around the classroom. School systems should receive monetary incentives for the number of students they graduate that are not fat. Government recognition of healthy fit kids should once again become a central concern of Health, Education, and Welfare.
Nutrition courses should be required at all grade levels. Schools should be rewarded for increasing the number of students who stay on campus and eat nutritious meals. Healthy snack breaks should be a part of daily school ritual at every level so that teachers can verbally reward students who actually eat their fruit. Tax payer money should not be spent on school lunch programs that compete with fast-food fare. Advertisements of non-nutritious foods—as has been done with alcoholic beverages and cigarettes–must be banned from television and certainly in the schools. Deals between schools and the soft drink industry must be ended.
Programs for adults must also be designed to provide incentives for not being fat. Providing discounts for drugs required because of conditions caused by obesity is counterproductive. Doing so not only fails to discourage weight gain, but it also ignores what studies show to be the number one medicine to prevent and treat common diseases. It does not come in a bottle. It is called exercise. Exercise, we now know, is superior t o Prozac for treating mild to moderate depression. Exercise can reverse certain kinds of heart disease and do away with the need for medicine to control blood sugar. Abundant research shows that even light weight-lifting can enable elderly people to get up out of their wheel chairs and walk after only few weeks. A proper diet and exercise can free many people with high blood pressure from medication. Something as simple as daily brisk walks can produce far more dramatic results than drugs in how fat and fit we are.
o Prozac for treating mild to moderate depression. Exercise can reverse certain kinds of heart disease and do away with the need for medicine to control blood sugar. Abundant research shows that even light weight-lifting can enable elderly people to get up out of their wheel chairs and walk after only few weeks. A proper diet and exercise can free many people with high blood pressure from medication. Something as simple as daily brisk walks can produce far more dramatic results than drugs in how fat and fit we are.
Ways for identifying people eligible for health discounts can be established. People who get a driver’s license must pass written and driving tests. Safe drivers and home owners get discounts on insurance. Similar systems can be set up to reward fit people when they apply for health insurance. A certificate from a doctor can show the results of blood tests, blood pressure readings and other health measures that indicate fitness. Scales can easily give readings on site. Just as cars are given a sticker showing they have passed inspection, centers of fitness and nutrition can be certified to provide evidence of completion of nutrition tests and other requirements that must be met for various levels of discount entitlement. Discounts for proven health supplements, as opposed to drugs to treat the maladies associated with obesity, can be awarded as part of the fitness incentive program. Obviously, such programs would demand universal fitness standards based on valid current research and updated upon discoveries in medical science. For example, safe limits for cholesterol need to be reviewed just as blood pressure limits have recently been changed for older folks.
Goals and measurements must be stated in language that confronts the negative consequences of our present behavior. As a communication specialist, I know that words influence behavior. We have to stop beating around the verbal bush. “Fat” and “obese” must be clearly defined and used openly to denote where we are and what we need to change. We must stop fooling ourselves and our children. Fat is not fun or funny or beautiful. Fat is costly and risky. And too often deadly.
The failure rate in managing our fatness and fitness has remained too high for too long. We don’t need to spend more tax dollars on helping people buy more drugs or use more health care. We should not be handing out tickets to help people end up in an early grave. Exercise is free and eating right can be done without extra cost. Doing both will save us all billions of health care dollars each year.
Federal intervention sounds like a nasty solution to some. To the contrary, it can be accomplished by built-in rewards for those of us who successfully assume greater personal responsibility for our health, nutrition, and fitness. And those of us who are already fit and healthy reap our rewards by not being forced to subsidize those who are not.
-0-
An award winning high school speech and English teacher, Priscilla Diffie-Couch went on to get her ED.D. from Oklahoma State University,  where she taught speech followed by two years with the faculty of communication at the University of Tulsa. In her consulting business later in Dallas, she designed and conducted seminars in organizational and group communication.
where she taught speech followed by two years with the faculty of communication at the University of Tulsa. In her consulting business later in Dallas, she designed and conducted seminars in organizational and group communication.
An avid tennis player, she has spent the last twenty years researching and reporting on health for family and friends. She has two children, four grandchildren and lives with her husband Mickey in The Woodlands, Texas.
-0-
A message from Bob Aronson. Bob’s Newheart was established to support and help everyone, but particularly those who need or have had organ transplants. Some of our blogs are specifically related to donation/transplantation issues while others are more general, but they are all related. Because anti-rejection drugs compromise immune systems, transplant recipients are more susceptible to a variety of diseases. We provide general health and medical information to help them protect themselves while at the same time, helping others live healthier lives and avoid organ failure.
Bob’s Newheart was established to support and help everyone, but particularly those who need or have had organ transplants. Some of our blogs are specifically related to donation/transplantation issues while others are more general, but they are all related. Because anti-rejection drugs compromise immune systems, transplant recipients are more susceptible to a variety of diseases. We provide general health and medical information to help them protect themselves while at the same time, helping others live healthier lives and avoid organ failure.
Bob’s Newheart mission is three-fold; 1) to provide news and information that promotes healthier living so people won’t need transplants; 2) To help recipients protect their new organs and; 3) to do what we can to ensure that anyone who needs an organ can get one. About 7,000 Americans die every year while waiting for a life-saving organ. I am sure you will agree that should not happen.
In the U.S. the great majority of people support organ donation, but only about 40% of us officially become organ donors. Many have good intentions but just don’t get around to it. It is hard to accept, but no one knows how long they will live. My transplanted heart came from a 30 year old man. I’m sure he had no intention of being a donor at that age. If you are not yet a donor, please register at www.donatelife.net it only takes a few seconds. Then, tell your family so there is no confusion when the time comes to donate. One organ donor can save or positively affect the lives of up to 60 people. There is no nobler thing you can do than becoming an organ donor.
Bob Aronson Founder of Bob’s Newheart Established November 3, 2007
Answers to the Most Common Health Questions
Author unknown but provided to us by Priscilla Diffie-Couch, E.d. D
Dr. Priscilla Diffie-Couch is my wife’s cousin and the health advisor to the entire Diffie family. Priscilla stays on top of the latest research and provides all of us with updates on a regular basis. Recently she sent the information you are about to read. She knows not where it originated but vouches for it’s accuracy. I think you will find these commonly asked questions and the answers most helpful.
Does olive oil prevent heart disease?

Short answer: Yes
The health benefits of olive oil come from the presence of polyphenols, antioxidants
That reduce the risk of heart diseases and cancers.
But to get these healthy compounds, consumers should buy good-quality, fresh “extra-virgin” olive oil, which has the highest polyphenol content. Most commercially available olive oils have low levels of polyphenols associated with poor harvesting methods, improper storage, and heavy processing.

Do cough syrups work?
Short answer: No
In 2006, the nation’s chest physicians agreed that the majority of over-the-counter cough medicines don’t actually work.
These colorful syrups typically contain doses of codeine and dextromethorphan that are too small to be effective.
Only cough suppressants that contain older antihistamines seem to relieve coughs.
That includes brompheniramine, an active ingredient in Dimetapp.

Do sugary soft drinks lead to diabetes?
Short answer: Yes
The majority of health research is stacked against sugar-sweetened soda. A large 2004 study in the Journal of the American Medical Association found that women who drank one or more sugary drinks per day increased their risk of developing type 2 diabetes by 83% compared to those who consumed less than one of these beverages per month.

Do I need sunscreen with more than 30 SPF?
Short answer: No
Sunscreens with an SPF (sun protection factor) of 30 block about 97% of ultraviolet rays,
While sunscreens with an SPF of higher than 30 block 97%-98%.
It’s more important that you choose “broad-spectrum” sunscreen, meaning it protects against both UVB and UVA rays.
Sunbathers also need to apply a generous amount of sunscreen in order to get the full benefit of the SPF.

Is the MSG in Chinese likely to give you a headache?
Short answer: No
A review of 40 years of clinical trials, published in the journal of the American Academy of Nurse Practitioners in 2006,
Found that all previous research “failed to identify a consistent relationship between the consumption of MSG
And the constellation of symptoms that comprise the syndrome,” including headaches and asthma attacks.
The misconception spawned from several poorly-done small studies in the 1960s that seemed to connect MSG with a variety of maladies that people experienced after eating at Chinese restaurants.
Learn more about the MSG myth here »

Do nuts make you fat?
Short answer: No
As much as 75% of a nut is fat. But eating fat doesn’t necessarily make you fat.
The bigger factor leading to weight gain is portion-size.
Luckily, nuts are loaded with healthy fats that keep you full. They’re also a good source of protein and fiber.
One study even found that whole almonds have 20% less calories than previously thought because
A lot of the fat is excreted from the body.

Is walking as effective as running?
Short answer: Yes
Studies have shown that how long you exercise — and thus how many calories you burn — is more important
Than how hard you exercise. Running is a more efficient form of exercise, but not necessarily better for you.
A six-year study published in the journal Arteriosclerosis, Thrombosis, and Vascular Biology in April found that walking at a moderate pace and running produced similar health benefits, so long as the same amount of energy was expended.

Is drinking fruit juice as good for you as eating fruit?
Short answer: No
Calorie for calorie, whole fruit provides more nutritional benefits than drinking the pure juice of that fruit.
That’s because when you liquefy fruit, stripping away the peel and dumping the pulp, many ingredients like
Fiber, calcium, vitamin C, and other antioxidants are lost.
For comparison, a five-ounce glass of orange juice that contains 69 calories has .3 grams of dietary fiber and 16 milligrams of calcium, whereas an orange with the same number of calories packs 3.1 grams of fiber and 60 milligrams of calcium.

Are all wheat breads better for you than white bread?
Short answer: No
Not all wheat breads are created equal. Wheat breads that contain all parts of the grain kernel,
Including the nutrient-rich germ and fiber-dense bran, must be labeled “whole grain” or “whole wheat.”
Some wheat breads are just white bread with a little bit of caramel coloring to make the bread appear healthier,
According to Reader’s Digest.

Can a hot tub make me sick?
Short answer: Yes
Hot tubs — especially ones in spas, hotels, and gyms — are perfect breeding grounds for germs.
The water is not hot enough to kill bacteria, but is just the right temperature to make microbes grow even faster.
Even though hot tubs are treated with chlorine, the heat causes the disinfectant to break down faster
than it would in regular pools.
The most common hot tub infection is pseudomonas folliculitis, which causes red, itchy bumps.
A more dangerous side-effect of soaking in a dirty Jacuzzi is a form of pneumonia known as Legionnaire’s disease.
This is what reportedly sickened more than 100 people at the Playboy Mansion back in 2011.

Does coffee cause cancer?
Short answer: No
Coffee got a bad rap in the 1980s when a study linked drinking coffee to pancreatic cancer.
The preliminary report was later debunked.
More recently, health studies have swung in favor of the caffeinated beverage.
Coffee has been linked to a lower risk of type 2 diabetes, Parkinson’s disease, liver cancer, and even suicide.

Do eggs raise cholesterol levels?
Short answer: No
Although egg yolks are a major source of cholesterol — a waxy substance that resembles fat — researchers have learned that saturated fat has more of an impact on cholesterol in your blood than eating foods that contain cholesterol.
“Healthy individuals with normal blood cholesterol levels should now feel free to enjoy foods like eggs in their diet every day,” the lead researcher from a 25-year University of Arizona study on cholesterol concluded.

Can you drink too much water?
Short answer: Yes
It is very rare for someone to die from drinking too much water, but it can happen.
Overhydrating is most common among elite athletes. Drinking an excess of water, called water intoxication, dilutes the concentration of sodium in the blood leading to a condition known as hyponatremia.
The symptoms of hyponatremia can range from nausea and confusion to seizures and even death in severe cases.
To avoid this, drink fluids with electrolytes during extreme exercise events.

Can yogurt ease digestive problems?
Short answer: Yes
Our digestive tract is filled with microorganisms — some good and some bad. Yogurt contains beneficial bacteria, generically called probiotics, that helps maintain a healthy balance.
Probiotics can relieve several gastrointestinal problems, including constipation and diarrhea.
Certain brands of yogurts, like Activa by Dannon, are marketed exclusively to treat tummy issues.

Do whitening toothpastes whiten teeth more than regular toothpastes?
Short answer: No
Whitening toothpastes usually contain peroxides and other strong abrasives that might make
your teeth appear whiter by removing stains. Unlike at-home whitening strips and gels that contain bleach,
these toothpastes do not actually change the color of your teeth.

Is it safe to microwave food in plastic containers?
Short answer: Yes
But the plastic container should display the words “microwave safe.” This means that the Food and Drug Administration has tested the container to make sure no chemicals used to make the plastic leech into foods during microwaving.
If chemicals do seep out into food, the amounts are tiny and not dangerous to our health.
As a general guideline, plastic grocery bags as well as most plastic tubs that hold margarine, yogurt, cream cheese,
and condiments are not microwave safe.

Can watching TV ruin your eyesight?
Short answer: No
Watching TV will not destroy your rods and cones as the outdated myth suggests. Before the 1950s,
TVs emitted radiation that could increase an individual’s risk of eye problems after excessive TV viewing.
Modern TVs have special shielding that blocks these harmful emissions.

Is red wine better for you than white wine?
Short answer: Yes
Red wine contains much more resveratrol than white wine, an antioxidant found in the skin of grapes
that has been shown to fight off diseases associated with aging.
 Is bottled water better for you than tap water?
Is bottled water better for you than tap water?
Short answer: No
Bottled water is no safer or purer than tap water, although it is substantially more expensive.
A recent study by Glasgow University in the U.K. found that bottled water is actually
more likely to be contaminated than water from your faucet because it is less well-regulated.
Bottled water and tap water typically come from the same sources — natural springs, lakes, and aquifers.
While public water supplies are tested for contaminants every day, makers of bottled water are only required
to test for specific contaminants every week, month, or year.
Dr. Priscilla Diffie-Couch will be a featured guest blogger from time to time on Bob’s Newheart. Watch for her posts and know that if Priscilla says it, you can depend on its accuracy.
Bob Aronson of Bob’s Newheart is a 2007 heart transplant recipient, the founder of Facebook’s nearly 4,000 member Organ Transplant Initiative (OTI) and the author of most of these donation/transplantation blogs. You may comment in the space provided or email your thoughts to me at bob@baronson.org. And – please spread the word about the immediate need for more organ donors. There is nothing you can do that is of greater importance. If you convince one person to be an organ and tissue donor you may save or positively affect over 60 lives. Some of those lives may be people you know and love.
Managing Your Health After an Organ Transplant
 When you become an organ transplant recipient your life changes. Not only does the quality of life improve but you have a new awareness of the importance of healthy living. Transplantable organs are in short supply and those of us who are fortunate enough to get one have a special obligation to take care of it. It is a gift of life that many never receive and your transplant center will make every effort to help you take care of yourself and your new organ. Follow their advice, eat healthy, live healthy and by all means, exercise as much as possible.
When you become an organ transplant recipient your life changes. Not only does the quality of life improve but you have a new awareness of the importance of healthy living. Transplantable organs are in short supply and those of us who are fortunate enough to get one have a special obligation to take care of it. It is a gift of life that many never receive and your transplant center will make every effort to help you take care of yourself and your new organ. Follow their advice, eat healthy, live healthy and by all means, exercise as much as possible.
I have researched and written the great majority of blogs that are published on Bob’s Newheart but not this one. It was researched and published by the American Society of Transplantation (AST). I only made some minor editing and formatting changes (the complete post can be found here– http://tinyurl.com/pcteky5).
This entry is longer than most because it offers critical information that you will need. It is not only comprehensive in scope, it is easy to understand and the principles are immediately and easily applicable. Please take the time to read and thoroughly consider every point. The information contained here can ensure not only a longer life but one of enhanced quality as well. And…while this post is meant for transplant recipients, the advice contained here will keep you healthy even if you haven’t had and don’t need an organ transplant.
KEEPING A HEALTHY OUTLOOK ON LIFE
After an organ transplant, there is hope for the future. However, there are a number of health concerns that you will face. For example, there is the chance that your new organ will not always function as well as it should. Transplant recipients also have a higher risk of developing certain conditions such as high blood pressure, high blood lipid levels, diabetes, kidney problems, liver problems, and bone disease. Infection and cancer are also conditions you need to keep in mind. Some conditions can affect any transplant recipient and some conditions are specific to the type of organ transplanted.
CARING FOR YOUR NEW ORGAN
Lab Tests for Measuring Organ Function
It is important to keep all of your scheduled checkups and lab appointments for monitoring organ function. Testing allows your transplant team to monitor the status of your transplant, detect rejection early, and start effective therapy right away.Common tests for checking organ function are listed below:
team to monitor the status of your transplant, detect rejection early, and start effective therapy right away.Common tests for checking organ function are listed below:
Liver function tests — Blood tests are used to monitor liver function (e.g. albumin); damage to liver cells (e.g., alanine transaminase [ALT], Aspartate transaminase [AST]) and some with conditions linked to the path by which bile is produced by the liver (e.g., gamma-glutamyl transferase and alkaline phosphatase)
· Pulmonary function tests — Tests like spirometry show how well you lungs are working
· Bronchoscopy — A test that uses an instrument (bronchoscope) to view the airways and diagnose lung disease
· Chest x-ray
· Upper and lower gastrointestinal (GI) endoscopies — These evaluations can detect abnormalities of your esophagus, stomach, and intestine
· Hemodynamic monitoring — Sonar-type echos may be used to detect high blood pressure in your heart and lungs or a catheter may be placed in the heart for periods of six to 12 hours
· Echocardiogram — Sonar-type echos can show abnormalities in the heart and lungs
· Electrocardiogram (EKG or ECG) — Asseses the electrical activity within your heart
· Renal function studies — Your doctor may ask you to collect your urine (usually for 24 hours) to evaluate if your kidneys are working properly. Blood tests such as serum creatinine are performed to measure kidney function
· Biopsy — A biopsy may also be taken to determine if a rejection episode has occurred. This is done by collecting a small piece of tissue from the organ and examining it under a microscope
OTHER HEALTH ISSUES
Anti-rejection medications increase your risk of developing certain conditions such as infection and cancer. Other side effects of some anti-rejection medications include high blood pressure, diabetes, high blood lipids, kidney disease, heart attack, stroke, and bone disease. Knowing the risks and taking steps now to prevent them is a good way to keep you and your new organ healthy.
HIGH BLOOD PRESSURE
High blood pressure (hypertension) is a common complication in patients who receive a transplant. High blood pressure can damage the arteries and the heart, increasing the risk of a stroke, a heart attack, kidney problems, or heart failure.For many patients, the cause of hypertension is not known. However, people with kidney disease, diabetes, or high blood pressure before the transplant are at higher risk of high blood pressure after the transplant. Other factors that contribute to high blood pressure after a transplant include a diet high in salt, clogged arteries, high blood lipid levels, smoking, obesity, and some anti-rejection medications such as cyclosporine, tacrolimus, and steroids (prednisone).
Recommended Blood Pressure Levels
People with a blood pressure of 140/90 mm Hg or higher are considered hypertensive. While most transplant recipients should have a blood pressure of 130/80 mm Hg, the ideal blood pressure can vary from person to person. The American Heart Association (AHA) guidelines for the target blood pressure in the general population can also be used as guidelines for organ transplant recipients. Normal blood pressure values for children are based on age, sex and height and in general are much lower than in adults.
- Normal Systolic (top) 120 Diastolic (bottom) 80
- Prehypertension Systolic 120-139, Diastolic 80-89
- Stage 1 hypertension Systolic 140-159, Diastolic 90-99
- Stage 2 hypertension Systolic 160 or higher, Diastolic 100 or higher
High blood pressure usually does not cause any symptoms so it is important to have your blood pressure checked by your transplant team at regular follow-up exams. Your transplant team may also want you to monitor your blood pressure closely while at home.
Reducing High Blood Pressure
- Making some lifestyle changes can lower your blood pressure and prevent hypertension
- Sometimes hypertension can be controlled with lifestyle changes such as diet and exercise, but most patients also require medication.
- There are a variety of medications for treating and controlling high blood pressure
- The most commonly prescribed medications include ACE inhibitors, ARBs, calcium channel blockers, beta-blockers, and diuretics. Some of these medications may have interactions with certain anti-rejection medications.
HIGH BLOOD LIPIDS
While lipids (cholesterol and related compounds) in your blood are necessary for good health, too high levels of some lipids can increase your risk of cardiovascular disease, a leading cause of death among transplant recipients. Most transplant recipients develop high blood lipids. Kidney, heart, and liver transplant patients usually display similar elevations in total cholesterol (TC) and low-density lipoprotein (LDL) cholesterol (“bad cholesterol”).Eating the wrong foods, lack of exercise, and being overweight can increase your risk of developing high levels of LDL cholesterol (“bad cholesterol”), high levels of triglycerides, and low levels of HDL cholesterol (“good cholesterol”). Transplant recipients who are obese, smoke cigarettes, or have high blood pressure are more likely to have high cholesterol. Steroids and some of the other anti-rejection medications, such as cyclosporine, sirolimus, and tacrolimus, can also cause high blood lipid levels.
Recommended Blood Lipid Levels
Be sure to ask your doctor what your cholesterol levels should be. In some instances, transplant recipients can follow target levels of blood lipids recommended in the National Cholesterol Education Program (NCEP) guidelines.
Lipid
Low
Optimal
High
LDL Cholesterol
100 mg/dL
160-189 mg/dL
HDL Cholesterol
40 mg/dL
60 mg/dL
Total Cholesterol
240 mg/dL
Reducing High Blood Lipid Levels
 Making healthy lifestyle changes can lower your chances of developing heart disease. You can help lower your blood lipid levels with a proper diet and regular exercise. A diet low in cholesterol and saturated fats may also help reduce your risk of coronary artery disease. In addition to making healthy changes to your diet, exercising for a minimum of 20 to 30 minutes 3 to 4 times a week can also reduce your lipid levels and lower your risk of heart attack or stroke. If you smoke, it is important that you STOP! If adjustment of your anti-rejection drugs, diet, and exercise are not successful in reducing lipid levels, your doctor may want you to take cholesterol-lowering medications. T
Making healthy lifestyle changes can lower your chances of developing heart disease. You can help lower your blood lipid levels with a proper diet and regular exercise. A diet low in cholesterol and saturated fats may also help reduce your risk of coronary artery disease. In addition to making healthy changes to your diet, exercising for a minimum of 20 to 30 minutes 3 to 4 times a week can also reduce your lipid levels and lower your risk of heart attack or stroke. If you smoke, it is important that you STOP! If adjustment of your anti-rejection drugs, diet, and exercise are not successful in reducing lipid levels, your doctor may want you to take cholesterol-lowering medications. T
Here are several medications that work to lower blood lipids. The most commonly prescribed medications are called statins, which include atorvastatin (Lipitor®), simvastatin (Zocor®), pravastatin (Pravachol®), fluvastatin (Lescol®), rosuvastatin (Crestor®), and lovastatin (Mevacor®). If your doctor prescribes a statin, you will need to be monitored for side effects because the risk of side effects is greater when taken with anti-rejection medications. You will also need blood tests to monitor liver and muscle function. Other types of medication that your transplant team might prescribe to treat high blood lipids include bile acid sequestrants, nicotinic acid, fibric acids, and cholesterol absorption inhibitors.
DIABETES
High blood glucose can cause many health problems, including diabetes, heart disease, kidney injury, nerve damage, and eye problems.Post-transplant diabetes (PTDM) is more common in transplant recipients who have a family history of diabetes as well as those who are overweight, are taking steroids, or have hepatitis C. Diabetes after a transplant is also more common among African Americans and some other ethnic groups such as Native Americans. Other risk factors for PTDM include older age of the recipient.
Controlling Blood Sugar Levels
Most transplant recipients with diabetes can follow the American Diabetes Association (ADA) guidelines. Patients with PTDM should establish a healthy (weight-reducing, if necessary) diet with a structured exercise program. A healthy diet is needed to prevent diabetes or to help control your glucose if diabetes does occur. For all transplant recipients, it is best to eat a healthy diet and exercise regularly to avoid weight gain and reduce the risk of developing high blood glucose or diabetes. Your transplant coordinator or dietician can help determine your recommended daily calorie intake. Limiting the amount of fats and sugar in your diet can also help to maintain a healthy level of blood glucose.
Treatment Options for Controlling Diabetes
There are several types of medications available for patients with diabetes. Depending on the level of glucose in your blood, treatment with oral hypoglycemic drugs and/or insulin may be indicated. For many transplant recipients, insulin injections or an insulin pump is an option for controlling blood sugar. Or, you may be given an oral medication to control blood glucose levels. Your transplant team will determine which medication is right for you.
KIDNEY DISEASE
Kidney function is often decreased in transplant recipients. This may be caused by a pre-existing condition such as diabetes, high blood pressure, or injury to the kidney before a transplant. Or it may be caused by medications used to prevent rejection after a transplant.The best way to help prevent kidney disease is to keep your blood pressure and blood glucose under control and to maintain a healthy weight. In addition, regular checkups with blood and urine tests will give your doctor important information for detecting early changes in kidney function and allowing appropriate steps to be taken.
BLOOD VESSELS DISEASE
Transplant recipients have a higher risk of developing blood vessel disease. Some anti-rejection medications increase the risk of high lipid levels, which can clog arteries and restrict the flow of blood to the heart and brain. Deposits — called atherosclerotic plaque — can completely or partially block blood vessels resulting in a myocardial infarction (heart attack) or acute coronary syndromes.Likewise, a stroke can occur if an artery that supplies blood to the brain becomes blocked. Partial blockage may temporarily reduce the blood supply to the brain. A complete loss of blood supply to the brain results in a stroke.
BONE DISEASE
Bone disease is a problem for many organ transplant recipients. Organ failure before your transplant may cause bones to become thin and brittle (osteoporosis). Other causes of osteoporosis include use of some anti-rejection drugs (corticosteroids), overactive parathyroid gland, cigarette smoking, and not enough calcium in your diet.
Preventing Bone Disease
There are some basic things you can do to help prevent or treat bone disease.
Exercise regularly, including weight lifting or strength training — be sure to discuss weight limits with your transplant team before beginning an exercise program
beginning an exercise program
Eat foods that are high in calcium, including low-fat yogurt, cheese, and milk
Choose foods and juices with calcium added
Get plenty of dietary protein (unless restricted by your doctor)
Take calcium supplements if directed by your doctor
Take vitamin D only as directed by your doctor
Stop smoking
Your doctor or transplant dietician will tell you if you need to take calcium or vitamin D supplements. Your doctor may also want you to take medications that prevent bone thinning, including bisphosphonates such as alendronate (Fosamax®), etidronate (Didrocal®), and risedronate (Actonel®) or calcitonin.
STAYING FIT
Diet – Things are shaping up
The recommended diet for transplant patients consists of 30% fats, 50% carbohydrates and 20% protein.
Your transplant dietician will give you specific instructions about your recommended daily allowance of specific nutrients. Some tips for following a healthy diet include:
Eat high-fiber foods such as raw fruits and vegetables
Increase your calcium intake by eating low-fat dairy products and green leafy vegetables or by taking calcium supplements (if directed by your doctor)
Eat less salt, processed foods, and snacks
Use herbs and spices to add flavor instead of salt
Drink plenty of water (unless you are told to limit fluids)
Eat as little fat and oil as possible
Eat high-protein foods such as lean meat, chicken (without the skin), fish, eggs, nuts (unsalted), and beans
Select healthier condiments such as mustard, low-fat mayonnaise, and low-fat salad dressing
Instead of frying, try baking, broiling, grilling, boiling, or steaming foods
Instead of using oil to cook, use nonstick, fat-free spray
Exercise
Exercise is a great way to help increase your energy and strength after a transplant. A regular exercise routine will also help you maintain your ideal weight, prevent high blood pressure and high lipid levels, and keep your bones strong. It also helps relieve stress and overcome feelings of depression.Soon after your transplant, you’ll want to start slow with a low-impact activity such as walking. With time, you can increase your workout with more demanding activities such as bicycling, jogging, swimming, or whatever exercise you enjoy. Training with dumbbells, cuff weights, or weights will increase strength and help prevent bone loss, but check with your transplant team first to determine how much weight is safe for you to lift. Stretching exercises are also important for muscle tone and flexibility. Be sure to check with your doctor before beginning or changing your exercise routine.
STOP Smoking
 Smoking also contributes to already high risk of cardiovascular, particularly in patients with diabetes and may be detrimental to kidney function. Transplant recipients who smoke should to STOP smoking as soon as possible.
Smoking also contributes to already high risk of cardiovascular, particularly in patients with diabetes and may be detrimental to kidney function. Transplant recipients who smoke should to STOP smoking as soon as possible.
Dental Care
Routine dental care is important both before and following transplantation as oral infections can cause significant medical problems and even death. According to the American Heart Association (AHA), pre-treatment with antibiotics is not needed for routine dental care unless the patient has an underlying heart condition that increases the risk of developing a heart infection. These include patients with heart transplants with graft valvulopathy (or a previous history of endocarditis, prosthetic valves, and certain forms of congenital heart diseases.)Gingival overgrowth (hypertrophy) is a dental issue that can arise in transplant patients especially those using cyclosporine. This occurrence of gingival overgrowth can be reduced by practicing good oral hygiene.
ROUTINE FOLLOW-UP EXAMS
All people should have regular exams to help prevent illness.
As we get older, there are some specific tests that should be done on a regular basis
Self-Monitoring
In addition to the tests that your transplant team will perform at regular follow-up visits, you will need to do some self-testing at home. Here are some things you will need to monitor:
Weight – Weigh yourself at the same time each day, preferably in the morning. If you gain 2 pounds in a day or more than 5 pounds total, call your transplant team.
Temperature – You should take your temperature daily, especially when you feel like you have a fever. Call your transplant team if your temperature is too high.
Blood pressure – Check your blood pressure as often as your transplant team recommends.
Pulse – You should check your pulse daily. A normal heart rate when not exercising should be 60 to 100 beats per minute. (If you have had a heart transplant, your resting heart rate may be as high as 110 to 120 beats per minute.)
Blood sugar – If you have high blood sugar or diabetes, you will need to monitor your blood sugar using a glucometer.
Do not take any pain medication (for example, Tylenol®, Motrin®, or Advil®), cold remedy, antacid, herbal medication, or any over-the-counter medication unless your transplant team tells you to.
PREGNANCY: BENEFITS AND RISKS
For female transplant recipients of child-bearing age, fertility is usually restored immediately after a transplant.
There have been thousands of births among women with transplanted organs.
Although pregnancy is now an expected part of the benefits afforded to women by organ transplantation, there are also a number of considerations. Getting pregnant is generally not recommended within the first year after a transplant because the doses of anti-rejection medications are highest; there is a greater risk of rejection; and many other medications are prescribed that are toxic to the developing fetus. Female transplant recipients of child-bearing age should continue using birth control until the doctor says that it is okay to get pregnant. Male transplant recipients may also be concerned about their ability to have children. Men may have fertility problems related to some transplant medications, but many men have been able to father healthy children after a transplant. If you are interested in, or thinking about, becoming pregnant you must talk to your transplant team first. Pregnancy should be planned when organ function and anti-rejection therapy are stable and there are no signs of rejection, high blood pressure, or infection.
High Risk Pregnancy
According to National Transplantation Pregnancy Registry (NTPR) over 70% of births to female transplant recipients are live births and most have favorable outcomes for child and mother. Although this success is encouraging, these pregnancies are still considered high risk. There are risks of complications during pregnancy for the transplant recipient as well as risk of infection and exposure to anti-rejection drugs for the fetus.For example, there is a greater risk of high blood pressure during pregnancy in the woman who has received a transplant. The risk of infection is higher for all transplant recipients, and urinary tract infections are the most common infections during pregnancy.
Other infections that may cause concern during pregnancy include herpes, hepatitis, toxoplasmosis, and cytomegalovirus. Other risks include preeclampsia and preterm delivery. The fetus is also at risk for infections such as cytomegalovirus and herpes simplex virus related to the suppression of the mother’s immune system by anti-rejection drugs. A common question is whether the baby born to a woman with a transplanted organ will be normal. We know that some babies are born premature to mothers with transplants and that they have low birth weights. It is not known whether there are long-term effects on the baby’s development. You should inform your baby’s pediatrician that your baby was exposed to anti-rejection drugs in the womb.
 There is a higher risk of birth defects with some anti-rejection drugs especially mycophenolate mofetil and azathioprine. The levels of anti-rejection drugs in the mother’s blood must be monitored closely. Monitoring of blood levels is particularly important in the third trimester, when fetal metabolism may increase the clearance of anti-rejection drugs from the blood. Ask your transplant team whether or not you should breast-feed. It is not known whether breast-feeding while on certain anti-rejection medications can harm the baby.
There is a higher risk of birth defects with some anti-rejection drugs especially mycophenolate mofetil and azathioprine. The levels of anti-rejection drugs in the mother’s blood must be monitored closely. Monitoring of blood levels is particularly important in the third trimester, when fetal metabolism may increase the clearance of anti-rejection drugs from the blood. Ask your transplant team whether or not you should breast-feed. It is not known whether breast-feeding while on certain anti-rejection medications can harm the baby.
A major concern for transplant recipients is whether pregnancy will lead to organ rejection or decreased function of the transplanted organ. In general, pregnancy does not affect organ function or patient survival as long your organ is working very well. But, it is very important to discuss with your transplant team whether or not a pregnancy will be too risky. Because pregnancy is considered high risk for transplant recipients, your transplant team may recommend and work with an obstetrician who specializes in high-risk pregnancies.
Bob Aronson of Bob’s Newheart is a 2007 heart transplant recipient, the founder of Facebook’s nearly 4,000 member Organ Transplant Initiative (OTI) and the author of most of these donation/transplantation blogs. You may comment in the space provided or email your thoughts to me at bob@baronson.org. And – please spread the word about the immediate need for more organ donors. There is nothing you can do that is of greater importance. If you convince one persBon to be an organ and tissue donor you may save or positively affect over 60 lives. Some of those lives may be people you know and love.
Initiative (OTI) and the author of most of these donation/transplantation blogs. You may comment in the space provided or email your thoughts to me at bob@baronson.org. And – please spread the word about the immediate need for more organ donors. There is nothing you can do that is of greater importance. If you convince one persBon to be an organ and tissue donor you may save or positively affect over 60 lives. Some of those lives may be people you know and love.
Sugar Could Be Killing us Physically and Financially
By Bob Aronson
 In September 2013, a bombshell report from Credit Suisse’s Research Institute brought into sharp focus the staggering health consequences of sugar on the health of Americans. The group revealed that approximately “30%–40% of healthcare expenditures in the USA go to help address issues that are closely tied to the excess consumption of sugar.” The figures suggest that our national addiction to sugar runs us an incredible $1 trillion in healthcare costs each year. The Credit Suisse report highlighted several health conditions including coronary heart diseases, type II diabetes and metabolic syndrome, which numerous studies have linked to excessive sugar intake.
In September 2013, a bombshell report from Credit Suisse’s Research Institute brought into sharp focus the staggering health consequences of sugar on the health of Americans. The group revealed that approximately “30%–40% of healthcare expenditures in the USA go to help address issues that are closely tied to the excess consumption of sugar.” The figures suggest that our national addiction to sugar runs us an incredible $1 trillion in healthcare costs each year. The Credit Suisse report highlighted several health conditions including coronary heart diseases, type II diabetes and metabolic syndrome, which numerous studies have linked to excessive sugar intake.
This blog is not meant to be a condemnation of sugar. It is a condemnation of our addiction to it. We all love a sweet taste and frankly, we deserve it from time to time. Often,there is no better reward, but we have to learn to limit our intake. Like so many things in life it is the abuse of any substance that can cause us to suffer. Sugar is particularly tough because it is unavoidable. It is in almost everything and often is a naturally occurring substance. We would all be a lot healthier if we would just read food labels and limit our excesses. Having established this little disclaimer, we can now discuss sugar and its potential and real dangers.
Women’s Health Magazine says that the typical American now swallows the equivalent of 22 sugar cubes every 24 hours. That means the average woman eats 70 pounds—nearly half her weight—of straight sugar every year. Women’s Health Magazine. http://www.womenshealthmag.com/health/dangers-of-sugar
In a major story on sugar Women’s Health goes on to say: When eaten in such vast quantities, sugar can wreak havoc on the body. Over time, that havoc can lead to diabetes and obesity, and also Alzheimer’s disease and breast, endometrial, and colon cancers. One new study found that normal-weight people who loaded up on sugar doubled their risk of dying from heart disease. Other research pinpoints excess sugar as a major cause of nonalcoholic fatty liver disease, which can lead to liver failure.
The magazine characterized the use of sugar this way, “The instant something sweet touches your tongue, your taste buds direct-message your  brain: deee-lish. Your noggin’s reward system ignites, unleashing dopamine. Meanwhile, the sugar you swallowed lands in your stomach, where it’s diluted by digestive juices and shuttled into your small intestine. Enzymes begin breaking down every bit of it into two types of molecules: glucose and fructose. Most added sugar comes from sugar cane or sugar beets and is equal parts glucose and fructose; lab-concocted high-fructose corn syrup, however, often has more processed fructose than glucose. Eaten repeatedly, these molecules can hit your body…hard.
brain: deee-lish. Your noggin’s reward system ignites, unleashing dopamine. Meanwhile, the sugar you swallowed lands in your stomach, where it’s diluted by digestive juices and shuttled into your small intestine. Enzymes begin breaking down every bit of it into two types of molecules: glucose and fructose. Most added sugar comes from sugar cane or sugar beets and is equal parts glucose and fructose; lab-concocted high-fructose corn syrup, however, often has more processed fructose than glucose. Eaten repeatedly, these molecules can hit your body…hard.
Anne Alexander, editorial director of Prevention and author of The Sugar Smart Diet provided this explanation of what sugars can do to your body.
Glucose
- It seeps through the walls of your small intestine, triggering your pancreas to secrete insulin, a hormone that grabs glucose from your blood and delivers it to your cells to be used as energy.
- But many sweet treats are loaded with so much glucose that it floods your body, lending you a quick and dirty high. Your brain counters by shooting out serotonin, a sleep-regulating hormone. Cue: sugar crash.
- Insulin also blocks production of leptin, the “hunger hormone” that tells your brain that you’re full. The higher your insulin levels, the hungrier you will feel (even if you’ve just eaten a lot). Now in a simulated starvation mode, your brain directs your body to start storing glucose as belly fat.
- Busy-beaver insulin is also surging in your brain, a phenomenon that could eventually lead to Alzheimer’s disease. Out of whack, your brain produces less dopamine, opening the door for cravings and addiction-like neurochemistry.
- Still munching? Your pancreas has pumped out so much insulin that your cells have become resistant to the stuff; all that glucose is left floating in your bloodstream, causing prediabetes or, eventually, full-force diabetes.
Fructose
- It, too, seeps through your small intestine into the bloodstream, which delivers fructose straight to your liver.
- Your liver works to metabolize fructose—i.e., turn it into something your body can use. But the organ is easily overwhelmed, especially if you have a raging sweet tooth. Over time, excess fructose can prompt globules of fat to grow throughout the liver, a process called lipogenesis, the precursor to nonalcoholic fatty liver disease.
- Too much fructose also lowers HDL, or “good” cholesterol, and spurs the production of triglycerides, a type of fat that can migrate from the liver to the arteries, raising your risk for heart attack or stroke.
- Your liver sends an S.O.S. for extra insulin (yep, the multi-tasker also aids liver function). Overwhelmed, your pancreas is now in overdrive, which can result in total-body inflammation that, in turn, puts you at even higher risk for obesity and diabetes
Robert Lustig, an endocrinologist from California gained national attention after a lecture he gave titled “Sugar: The Bitter Truth” went viral in 2009. www.youtube.com/watch?v=dBnniua6-oM
Lustig’s research looked at the connection between sugar consumption and the poor health of Americans came to a conclusion that startled many. The Doctor has published twelve articles in peer-reviewed journals identifying sugar as a major factor in the epidemic of degenerative disease that now afflicts our country. Lustig’s data clearly show that excessive sugar consumption is a key player in the development of some cancers along with obesity, type II diabetes, hypertension, and heart disease. As a result he has concluded that 75% of all diseases in America are brought on by our lifestyle and are entirely preventable.
While most in the medical profession seem to accept Lustig’s assessment of sugar at least one MD David Katz the director of the Yale Prevention Center, disagrees. http://www.huffingtonpost.com/david-katz-md/sugar-health-evil-toxic_b_850032.html Katz says, among other things, “So those most motivated to get the sugar they need wind up getting the most sugar. They, in turn, benefit from this by having more of the needed food energy — and thus are more likely to survive. In particular, they are more likely to survive into adulthood, and to procreate. And thus they become our ancestors, who pass traits along to us.”
Lest you think I am making a mountain of a molehill allow some of the body of evidence that sugar can cause health problems. The claims about the ill health effects of sugar are not just those leveled by Dr. Lustig, they are backed by a solid body of research. Here are just a few of the research headlines.
- Consumption of Sugar-Sweetened Drinks Linked to Heart Disease
- How Fructose Causes Obesity and Diabetes
- Fructose intake connected with an increased risk of cardiovascular illness and diabetes in teenagers
- Fructose consumption increases the risk of heart disease.
- The Negative Impact of Sugary Drinks on Children.
- Sugar and High Blood Pressure
- Sugar Consumption Associated with Fatty Liver Disease and Diabetes
- The Adverse Impact of Dietary Sugars on Cardiovascular Health
- Rats Fed High Fructose Corn Syrup Exhibit Impaired Brain Function
- High Fructose Corn Syrup Intake Linked with Mineral Imbalance and Osteoporosis.
- Diet of Sugar and Fructose Impairs Brain Function
To be healthy and avoid sugar or at least limit your intake you simply must read labels. Unfortunately those who seek to force sugar into our systems have found many ways of complying with the law and telling us there’s sugar in their food but they do it in a manner that sounds less menacing.
SWEET SYNONYMS
Watch for these sneaky ingredients when reading food labels. Some sound scientific, some almost healthy—but in the end, they all mean “sugar.”
Agave Nectar
Barbados Sugar
Barley Malt Syrup
Beet Sugar
Blackstrap Molasses
Cane Crystals
Cane Juice Crystals
Castor Sugar
Corn Sweetener
Corn Syrup
Corn Syrup Solids
Crystalline Fructose
Date Sugar
Demerara Sugar
Dextrose
Evaporated Cane Juice
Florida Crystals
Fructose
Fruit Juice
Fruit Juice Concentrate
Galactose
Glucose
Glucose Solids
Golden Sugar
Golden Syrup
Granulated Sugar
Grape Juice Concentrate
Grape Sugar
High-Fructose Corn Syrup
Honey
Icing Sugar
Invert Sugar
Lactose
Malt Syrup
Maltodextrin
Maltose
Mannitol
Maple Syrup
Molasses
Muscovado Syrup
Organic Raw Sugar
Powdered Sugar
Raw Sugar
Refiners’ Syrup
Rice Syrup
Sorbitol
Sorghum Syrup
Sucrose
Table Sugar
Treacle
Turbinado Sugar
Yellow Sugar
PICK YOUR POISON
Ultimately, added sugar is added sugar—it all affects you roughly the same way, regardless of where it comes from. Below you will find a short list of the most active and dangerous evil doers. .
High-Fructose Corn Syrup (HFCS)

Derived from corn starch, syrupy HFCS might be the scariest sweet. Much of it contains mercury, a by-product of chemical processing. But another danger is its high artificial fructose content, not to mention that it can be 75 times sweeter than white sugar. (Listen up, agave eaters: The processed nectar can be up to 85 percent fructose and possibly more damaging to your liver than HFCS!)
Honey (http://tinyurl.com/ogge3r6

Often touted as far healthier than refined sugar, these do contain fewer chemicals and a better glucose-fructose balance (plus a few helpful antioxidants). However, says Anne Alexander, author of The Sugar Smartdiet even if the unique flavors of maple syrup and raw honey may lead people to use less, these sweeteners can still spike the body.
Natural Sugar

Sweet news! Unless it’s all you eat, it’s hard to go overboard on truly natural sugars that come directly from fruits and some veggies. Here’s the trick: You have to actually eat the produce. Fruit juices, even those without added sweeteners, will still sugar-bomb your bloodstream. The key is in the fiber, which slows sugar’s absorption in your body, preventing an insulin spike. Any fruit is fair game. “Ones with the most natural sugar have the most fiber,” says Robert Lustig, M.D.
So what’s the bottom line? Should we avoid sugar completely? Is that even possible? Are sugar substitutes a healthy alternative?
First, you probably cannot avoid sugar completely and still eat because it appears naturally in so much of our daily diet. Additionally, sugar is added to almost every product on the supermarket shelves so the best you can do is severely limit the amount you consume. Here’s what the Mayo Clinic says. http://www.mayoclinic.org/healthy-living/nutrition-and-healthy-eating/in-depth/added-sugar/art-20045328
How to reduce added sugar in your diet
To reduce the added sugar in your diet, try these tips:
- Drink water or other calorie-free drinks instead of sugary, nondiet sodas or sports drinks. That goes for blended coffee drinks, too.
- When you drink fruit juice, make sure it’s 100 percent fruit juice — not juice drinks that have added sugar. Better yet, eat the fruit rather than juice.
- Choose breakfast cereals carefully. Although healthy breakfast cereals can contain added sugar to make them more appealing to children, plan to skip the non-nutritious, sugary and frosted cereals.
- Opt for reduced-sugar varieties of syrups, jams, jellies and preserves. Use other condiments sparingly. Salad dressings and ketchup have added sugar.
- Choose fresh fruit for dessert instead of cakes, cookies, pies, ice cream and other sweets.
- Buy canned fruit packed in water or juice, not syrup.
- Snack on vegetables, fruits, low-fat cheese, whole-grain crackers and low-fat, low-calorie yogurt instead of candy, pastries and cookies.
The final analysis
By limiting the amount of added sugar in your diet, you can cut calories without compromising on nutrition. In fact, cutting back on foods with added sugar and solid fats may make it easier to get the nutrients you need without exceeding your calorie goal.
Mayo concludes it’s summary on sugary by saying, “Take this easy first step: Next time you’re tempted to reach for a soda or other sugary drink, grab a glass of ice-cold water instead.”
Artificial sweeteners

“So if I am supposed to avoid sugar, but I like sweets what are my alternatives?” Well, there’s a lot of controversy surrounding this topic so we’ll turn to Web MD for an answer. http://www.webmd.com/food-recipes/features/best-sugar-substitutes
Thanks to the newest sugar substitutes, it’s becoming easier (and healthier) to bake your cake and eat it too!
There are so many alternative sweeteners available now that they seem to be elbowing sugar right off the supermarket shelf. But what’s so wrong with sugar? At just 15 calories per teaspoon, “nothing–in moderation,” says Lona Sandon, R.D., an assistant professor of clinical nutrition at the University of Texas Southwestern Medical Center in Dallas. “The naturally occurring sugar in an apple is fine, but if we can reduce some of the added sugar in our diet, we can remove some of the empty calories.” Less than 25 percent of your daily calories should come from the added sugar in foods like cookies, cereal, and ketchup, she says. To satisfy your sweet tooth–especially if you’re counting calories, limiting carbs, or dealing with diabetes–try these options:
SWEETLEAF AND TRUVIA
What they are: These sugar alternatives are the latest made from stevia, an herb found in Central and South America that is up to 40 times sweeter than sugar but has zero calories and won’t cause a jump in your blood sugar. Stevia was slow to catch on because of its bitter, licorice-like aftertaste, but makers of Truvia and SweetLeaf have solved this problem by using the sweetest parts of the plant in their products.
Where to find them: In grocery stores and natural-food stores throughout the country and online at sweetleaf.com and truvia.com.
Health Rx: “Truvia’s one of the most promising alternatives out there,” says nutritionist Jonny Bowden, Ph.D., author of The Healthiest Meals on Earth . “Right now, it looks safe. It tastes just like sugar and has almost no glycemic index, which means it won’t spike your blood sugar.”
WHEY LOW
What it is: Three naturally occurring sugars–fructose, the sugar in fruit; sucrose, or table sugar; and lactose, the sugar in milk–are blended to create this sweetener. While individually the sugars are fully caloric, when blended in Whey Low they interact in such a way that they aren’t completely absorbed into the body. As a result, at four calories per teaspoon, Whey Low has one quarter of the calories and less than one third of the glycemic index of sugar, so you’re less likely to crash after consuming it. It’s available in varieties similar to granular sugar, brown sugar, maple sugar, and confectioners’ sugar.
 Bob Aronson of Bob’s Newheart is a 2007 heart transplant recipient, the founder of Facebook’s nearly 4,000 member Organ Transplant Initiative (OTI) and the author of most of these donation/transplantation blogs. You may comment in the space provided or email your thoughts to me at bob@baronson.org. And – please spread the word about the immediate need for more organ donors. There is nothing you can do that is of greater importance. If you convince one person to be an organ and tissue donor you may save or positively affect over 60 lives. Some of those lives may be people you know and love.
Bob Aronson of Bob’s Newheart is a 2007 heart transplant recipient, the founder of Facebook’s nearly 4,000 member Organ Transplant Initiative (OTI) and the author of most of these donation/transplantation blogs. You may comment in the space provided or email your thoughts to me at bob@baronson.org. And – please spread the word about the immediate need for more organ donors. There is nothing you can do that is of greater importance. If you convince one person to be an organ and tissue donor you may save or positively affect over 60 lives. Some of those lives may be people you know and love.
Vitamin Supplements — May Not Be Necessary and They Could Harm You
By Bob Aronson
 The National Institutes of Health (NIH) says Americans have been taking multivitamin/mineral (MVM) supplements since the early 1940s, when the first such products became available. MVMs are still popular dietary supplements and, according to estimates, more than one-third of all Americans take them. MVMs account for almost one-fifth of all purchases of dietary supplements.
The National Institutes of Health (NIH) says Americans have been taking multivitamin/mineral (MVM) supplements since the early 1940s, when the first such products became available. MVMs are still popular dietary supplements and, according to estimates, more than one-third of all Americans take them. MVMs account for almost one-fifth of all purchases of dietary supplements.
“You have to get your vitamins.” I’ve heard that phrase since I was a child, but why? What are Vitamins and are vitamin pills or supplements the same as the vitamins found naturally in what we eat and in sunshine? Vitamins are not all the same. There can be a huge difference between those that are naturally contained in our food and the sometimes “smelly” things that come in a bottle from your Pharmacy.
Over the past several years there have been a number of news reports about vitamins. Some experts support their use, some say the supplements are worthless and others say they can actually cause harm. What’s true? All of the above! We’ll try to shed some light on the subject so let’s start with their importance to our health.
Vitamin deficiencies lead to a wide range of problems spanning from anorexia to obesity, organ malfunction, confusion, depression and fatigue. We need vitamins. The question that must be answered is; how do you know which ones? We’ll provide an answer.
Tough question when you consider the fact that the NIH says, “No standard or regulatory definition is available for an MVM supplement—![]() such as what nutrients it must contain and at what levels. Therefore, the term can refer to products of widely varied compositions and characteristics. These products go by various names, including multis, multiples, and MVMs. Manufacturers determine the types and levels of vitamins, minerals, and other ingredients in their MVMs. As a result, many types of MVMs are available in the marketplace.”
such as what nutrients it must contain and at what levels. Therefore, the term can refer to products of widely varied compositions and characteristics. These products go by various names, including multis, multiples, and MVMs. Manufacturers determine the types and levels of vitamins, minerals, and other ingredients in their MVMs. As a result, many types of MVMs are available in the marketplace.”
It is entirely possible that there are no standards because the vitamin industry is huge and can afford heavy lobbying to ensure that they remain free of government regulation. The NIH says that sales of all dietary supplements in the United States totaled an estimated $30.0 billion in 2011. This amount included $12.4 billion for all vitamin- and mineral-containing supplements, of which $5.2 billion was for MVMs. If the government set standards, every single manufacturer would have to reformulate their products to meet them. Doing so would be costly so there is no wonder that the industry would rather not rock their very profitable boat.
 Whether your vitamins are hurting you is another story. What people are not aware of is that all vitamins are not created equal, and most are actually synthetic and the synthetic vitamins are rarely like the real thing.
Whether your vitamins are hurting you is another story. What people are not aware of is that all vitamins are not created equal, and most are actually synthetic and the synthetic vitamins are rarely like the real thing.
The type of vitamins that benefit us most is murky but there are some. However, a healthy diet should provide most of the nutrients our bodies need. Sometimes, though, supplements can help. The problem is, which ones? How do you know what to buy?
For the most part, medical science has made it clear that most vitamin supplements are either useless or cause harm and we’ll elaborate on those claims shortly. First, though, you ought to know what’s good for you and what seems to work for some conditions.
This article in Smithsonian.com lists five supplements that can be helpful. http://www.smithsonianmag.com/science-nature/five-vitamins-and- supplements-are-actually-worth-taking-180949735/#VsZOfYrBAkvtVYvY.99
supplements-are-actually-worth-taking-180949735/#VsZOfYrBAkvtVYvY.99
Of all the “classic” vitamins—the vital organic compounds discovered between 1913 and 1941 and termed vitamin A, B, C, etc.—vitamin D is by far the most beneficial to take in supplement form. Researchers found that adults who took vitamin D supplements daily lived longer than those who didn’t.
Other research has found that in kids, taking vitamin D supplements can reduce the chance of catching the flu, and that in older adults, it can improve bone health and reduce the incidence of fractures.
Probiotics
A mounting pile of research is showing how crucial the trillions of bacterial cells that live inside us are in regulating our health, and how harmful it can be to suddenly wipe them out with an antibiotic. Thus, it shouldn’t come as a huge surprise that if you do go through a course of antibiotics, taking a probiotic (either a supplement or a food naturally rich in bacteria, such as yogurt) to replace the bacteria colonies in your gut is a good idea.
In 2012, a meta-analysis of 82 randomized controlled trials found that use of probiotics significantly reduced the incidence of diarrhea after a course of antibiotics.
All the same, probiotics aren’t a digestive cure-all: they haven’t been found to be effective in treating irritable bowel syndrome, among other chronic ailments. Like most other supplements that are actually effective, they’re useful in very specific circumstances, but it’s not necessary to continually take them on a daily basis.
Zinc
Vitamin C might not do anything to prevent or treat the common cold, but the other widely-used cold supplement, zinc, is actually worth taking. A mineral that’s involved in many different aspects of your cellular metabolism, zinc appears to interfere with the replication of rhinoviruses, the microbes that cause the common cold.
This has been borne out in a number of studies
Niacin
Also known as vitamin B3, niacin is talked up as a cure for all sorts of conditions (including high cholesterol, Alzheimer’s, diabetes and headaches) but in most of these cases, a prescription-strength dose of niacin has been needed to show a clear result.
At over-the-counter strength, niacin supplements have only been proven to be effective in helping one group of people: those who have heart disease. A 2010 review found that taking the supplement daily reduced the chance of a stroke or heart attack in people with heart disease, thereby reducing their overall risk of death due to a cardiac
Garlic
Garlic, of course, is a pungent herb. It also turns out to be an effective treatment for high blood pressure when taken as a concentrated supplement.
A 2008 meta-analysis of 11 randomized controlled trials (in which similar groups of participants were given either a garlic supplement or placebo, and the results were compared) found that, on the whole, taking garlic daily reduced blood pressure, with the most significant results coming in adults who had high blood pressure at the start of the trials.
On the other hand, there have also been claims that garlic supplements can prevent cancer, but the evidence is mixed.
Vitamin Supplements are unnecessary and may cause harm.
In December of last year, the Annals of Internal Medicine reported that, “Not only are the pills mostly unnecessary, but they could actually do![]() harm those taking them. We believe that the case is closed—supplementing the diet of well-nourished adults with (most) mineral or vitamin supplements has no clear benefit and might even be harmful. These vitamins should not be used for chronic disease prevention. Enough is enough.” http://www.cbsnews.com/news/multivitamin-researchers-say-case-is-closed-supplements-dont-boost-health/
harm those taking them. We believe that the case is closed—supplementing the diet of well-nourished adults with (most) mineral or vitamin supplements has no clear benefit and might even be harmful. These vitamins should not be used for chronic disease prevention. Enough is enough.” http://www.cbsnews.com/news/multivitamin-researchers-say-case-is-closed-supplements-dont-boost-health/
Based on three studies examining multivitamins’ links to cancer prevention, heart health, and cognitive function, the research is a blow to the multi-billion dollar industry that produces them and to the millions of Americans who religiously shell out their dollars for false hope.
The doubts about vitamin supplements are not new. In his 2013 book Do You Believe in Magic, Dr. Paul Offit pointed to a handful of major studies over the past five years that showed vitamins have made people less healthy. “In 2008, a review of all existing studies involving more than 230,000 people who did or did not receive supplemental antioxidants found that vitamins increased the risk of cancer and heart disease.”
Last year, researchers published new findings from the Women’s Health Initiative, a long-term study of more than 160,000 midlife women. The data showed that multivitamin-takers are no healthier than those who don’t pop the pills, at least when it comes to the big diseases—cancer, heart disease, stroke. “Even women with poor diets weren’t helped by taking a multivitamin,” says study author Marian Neuhouser, PhD, in the cancer prevention program at the Fred Hutchinson Cancer Research Center, in Seattle.
That said, there is one group that probably ought to keep taking a multi-vitamin: women of reproductive age. The supplement is insurance in case of pregnancy. A woman who gets adequate amounts of the B vitamin folate is much less likely to have a baby with a birth defect affecting the spinal cord.
The problem is that many vitamin and mineral supplements are manufactured synthetically. Some estimates place the amount at 90 percent and higher and while they are made to mimic natural vitamins they are not the same. Natural vitamins come directly from plants and animals, they are not produced in a lab and — most synthetic vitamins lack co-factors associated with naturally-occurring vitamins because they have been “isolated.”
Isolated vitamins can’t always be used by the body, and are either stored or excreted. Most synthetic vitamins don’t have the necessary trace minerals either and must use the body’s own mineral reserves which can then cause mineral deficiencies.
Most synthetic supplements contain chemicals that do not occur in nature. The history of the human race is such that our bodies have grown accustomed to consuming the food we grow and gather naturally, from the earth, not food that is synthesized in a lab.
![]() Web MD offers this assessment.
Web MD offers this assessment.
What Vitamin and Mineral Supplements Can and Can’t Do
http://www.webmd.com/vitamins-and-supplements/nutrition-vitamins-11/help-vitamin-supplement
By Kathleen M. Zelman, MPH, RD, LD
Reviewed By Elizabeth Ward, MS, RD
Experts say there is definitely a place for vitamin or mineral supplements in our diets, but their primary function is to fill in small nutrient gaps. They are “supplements” intended to add to your diet, not take the place of real food or a healthy meal plan.
WebMD takes a closer look at what vitamin and mineral supplements can and cannot do for your health.
Food First, Then Supplements
Vitamins and other dietary supplements are not intended to be a food substitute. They cannot replace all of the nutrients and  benefits of whole foods.
benefits of whole foods.
“They can plug nutrition gaps in your diet, but it is short-sighted to think your vitamin or mineral is the ticket to good health — the big power is on the plate, not in a pill,” explains Roberta Anding, MS, RD, a spokesperson for the American Dietetic Association and director of sports nutrition at Texas Children’s Hospital in Houston.
It is always better to get your nutrients from food, agrees registered dietitian Karen Ansel. “Food contains thousands of phytochemicals, fiber, and more that work together to promote good health that cannot be duplicated with a pill or a cocktail of supplements.”
What Can Vitamin and Mineral Supplements Do for Your Health?
When the food on the plate falls short and doesn’t include essential nutrients like calcium, potassium, vitamin D, and vitamin B12, some of the nutrients many Americans don’t get enough of, a supplement can help take up the nutritional slack. Vitamin and mineral supplements can help prevent deficiencies that can contribute to chronic conditions.
Numerous studies have shown the health benefits and effectiveness of supplementing missing nutrients in the diet. A National Institutes of Health (NIH) study found increased bone density and reduced fractures in postmenopausal women who took calcium and vitamin D.
Beyond filling in gaps, other studies have demonstrated that supplemental vitamins and minerals can be advantageous. However, the exact benefits are still unclear as researchers continue to unravel the potential health benefits of vitamins and supplements.
Web MD offers these tips to guide your vitamin and mineral selection:
- Think nutritious food first, and then supplement the gaps. Start by filling your grocery cart with a variety of nourishing, nutrient-rich foods. Use the federal government’s My Plate nutrition guide to help make sure your meals and snacks include all the parts of a healthy meal.
- Take stock of your diet habits. Evaluate what is missing in your diet. Are there entire food groups you avoid? Is iceberg lettuce the only vegetable you eat? If so, learn about the key nutrients in the missing food groups, and choose a supplement to help meet those needs. As an example, it makes sense for anyone who does not or is not able to get the recommended three servings of dairy every day to take a calcium and vitamin D supplement for these shortfall nutrients.
- When in doubt, a daily multivitamin is a safer bet than a cocktail of individual supplements that can exceed the safe upper limits of the recommended intake for any nutrient. Choose a multivitamin that provides 100% or less of the Daily Value (DV) as a backup to plug the small nutrient holes in your diet.
- Are you a fast food junkie? If your diet pretty much consists of sweetened and other low-nutrient drinks, fries, and burgers, then supplements are not the answer. A healthy diet makeover is in order. Consult a registered dietitian.
- Respect the limits. Supplements can fill in where your diet leaves off, but they can also build up and potentially cause toxicities if you take more than 100% of the DV.
- Most adults and children don’t get enough calcium, vitamin D, or potassium according to the 2010 Dietary Guidelines. Potassium-rich foods, including fruits, vegetables, dairy, and meat are the best ways to fill in potassium gaps. Choose an individual or a multivitamin supplement that contains these calcium and vitamin D as a safeguard.
- The best way to judge any supplement or medication is by reviewing clinical trials. There aren’t a lot of them done on vitamins,
 but those that have been conducted are quite revealing. The NIH concluded that most supplements not only don’t work as intended, they actually make things worse. They examined the efficacy of 13 vitamins and 15 essential minerals as reported in long-term, randomized clinical trials and there were some positive results like:
but those that have been conducted are quite revealing. The NIH concluded that most supplements not only don’t work as intended, they actually make things worse. They examined the efficacy of 13 vitamins and 15 essential minerals as reported in long-term, randomized clinical trials and there were some positive results like: - A combination of calcium and vitamin D was shown to increase bone mineral density and reduce fracture risk in postmenopausal women.
- There was some evidence that selenium reduces risk of certain cancers.
- Vitamin E maydecrease cardiovascular deaths in women and prostate cancer deaths in male smokers.
- Vitamin D showed some cardiovascular benefit.

Those few positives are overwhelmed by the negative findings.
- Trials of niacin (B3), folate, riboflavin (B2), and vitamins B6 and B12 showed no positive effect on chronic disease occurrence in the general population
- There was no evidence to recommend beta-carotene and some evidence that it may cause harm in smokers.
- High-dose vitamin E supplementation increased the risk of death from all causes.
So what’s the bottom line? Our research indicates that most medical authorities pretty much dismiss the usefulness of most vitamin supplements. Most revealing, though, and also dangerous is the fact that there are no standards for vitamin supplements. The companies that make them can each have their own formulations and there is no approval process so the consumer may be at great risk. Buyer beware. Don’t believe the advertising. If you are determined to take these supplements, though, google them and look for clinical trials. If there are none, don’t buy. If there are, read them carefully. For the most part the best advice is, save your money because most of us don’t have a clue as to what we are buying.
Bob Aronson of Bob’s Newheart is a 2007 heart transplant recipient, the founder of Facebook’s nearly 4,000 member Organ Transplant
 Initiative (OTI) and the author of most of these donation/transplantation blogs. You may comment in the space provided or email your thoughts to me at bob@baronson.org. And – please spread the word about the immediate need for more organ donors. There is nothing you can do that is of greater importance. If you convince one person to be an organ and tissue donor you may save or positively affect over 60 lives. Some of those lives may be people you know and love.
Initiative (OTI) and the author of most of these donation/transplantation blogs. You may comment in the space provided or email your thoughts to me at bob@baronson.org. And – please spread the word about the immediate need for more organ donors. There is nothing you can do that is of greater importance. If you convince one person to be an organ and tissue donor you may save or positively affect over 60 lives. Some of those lives may be people you know and love.
Aspartame (Equal/Nutri-Sweet) Is NOT The Killer in Your Fridge
By Bob Aronson
Bob is the founder of this blog and the primary author. He receives no monetary or other outside support nor does he allow anyone to see or review his posts before publication. The topics are known only to him until they are published.

This post is NOT an endorsement of Aspartame nor does it encourage its use. Neither sugar nor their substitutes promote good health. This is a response to the inaccurate and scientifically unverifiable claims leveled against Aspartame, but just because we found those claims to be false, readers should not assume we recommend its use. We do not. If you think it is dangerous — don’t use it.
If you want more information about sugar and sugar substitutes read our blog on the subject here. https://bobsnewheart.wordpress.com/2014/08/05/sugar-could-be-killing-us-physically-and-financially/ Please note, that this blog also does not recommend Aspartame as a sugar substitute.
Aspartame is NOT the Killer In Your Fridge!
There is a blog making the rounds that insists that Aspartame (Equal or Nutri-sweet) the sweetener found in most diet drinks is not only dangerous but deadly. “Aspartame, A killer in Your Fridge” pretends to have evidence but it is all circumstantial and doesn’t hold up under close scrutiny. I’ll explain more in a bit.
The blog disturbed me because as a transplant recipient I know how careful we have to be to protect ourselves from any number of real threats to our health. Threats like skin and other cancers, viruses and brittle bones. Our compromised immune systems are susceptible to some terrible afflictions and we just don’t need the added stress of worrying about imaginary threats supported by “Junk science” and spread by rumor, innuendo and incomplete or inadequate research. That’s why I’m writing this blog.
Let me start by getting right to the point. There is no solid evidence that Aspartame is any more harmful than the carbonation in your favorite soft drink. No Solid Evidence! There is anecdotal evidence but that’s kind of like hearsay in a courtroom. The scientific community rejects it. They prefer to make decisions based on real and proven scientific examination that studies foods, drugs and other items in a manner that leaves little or no doubt.
The “Gold Standard” of scientific examination is the double blind placebo study. Here’s the simplest explanation I could find:
A placebo is the term for a dummy drug or a substance that looks, smells and tastes like the item that is being studied, but which has no active ingredient. It is given to a patient in place of the substance under investigation. Clinical trials show that between 30% to 40% of people will show improvement when given a placebo because they believe it will work.
In drug trials, a control group is given a placebo while another group is given the drug being studied. That way, researchers can compare the drug’s effectiveness against the placebo’s effectiveness.
Using a placebo helps find out whether the active drug is really active. It also helps interpret side effects. For example, if 10% of people in the active drug group report having a headache and 2% of people in the placebo group report a headache, then it is reasonable to think that the active drug can cause headaches.
If 10% of the placebo group also reported a headache, then it is reasonable to think that the active drug doesn’t cause a headache.
A double-blinded placebo study is where neither the administrators of the study nor the patients know which group the patient is in.
Blinding prevents different care or treatment being given based on the personal beliefs of either the doctor or patient. A double-blind procedure is used to guard against both experimenter bias and placebo effects. The blog in question is not based on double blind placebo studies. It is all circumstance and speculation and totally without foundation.
The “Killer in Your Fridge” blog cites Individual cases where a person or even several persons appear to be affected is classified as anecdotal because there is no control group and because of the high probability of coincidence. An example is, “My son got a vaccination and is now autistic.” To many that sounds like real evidence. It isn’t and that’s what the author of the “Killer in your Fridge” blog, continues to cite over and over again. It does not offer one scintilla of scientific evidence that aspartame is harmful. When you skim away the sensationalism and look for proof you will find nothing more than speculation based on coincidence.
Make no mistake, we are not endorsing artificial sweeteners. Just because something is approved as “safe for human consumption” doesn’t mean we should consume it. While my research has not revealed any real dangers in consuming artificial sweeteners it also did not reveal a single benefit. With that introduction here’s more detail on exactly what prompted me to write this blog.
 A few days ago I got an email that included a post titled “A Killer in Your Fridge ~ Sweet Poison…A MUST READ.” Being as I regularly report on health issues the headline got my attention so I read the blog which at first glance made a convincing case for establishing Aspartame the artificial sweetener as a killer of thousands maybe millions of people. But something about the blog struck me as wrong.
A few days ago I got an email that included a post titled “A Killer in Your Fridge ~ Sweet Poison…A MUST READ.” Being as I regularly report on health issues the headline got my attention so I read the blog which at first glance made a convincing case for establishing Aspartame the artificial sweetener as a killer of thousands maybe millions of people. But something about the blog struck me as wrong.
I put down my Diet Mountain Dew, cleaned my glasses with a microfiber cloth and began to read the blog again. On my second, more thorough read I found what I considered to be huge holes in the logic and a lack of solid scientific evidence. You can reach your own conclusions by reading the blog at http://rhondagessner.wordpress.com/2013/09/02/a-killer-in-your-fridge-sweet-poison-a-must-read/
A lot of what you read in the blog sounds quite convincing but upon close examination one finds that most of the so-called evidence is anecdotal meaning that the author points to one or two or even several people who contracted a certain illness and who also happened to be consuming aspartame in some form at the time. While interesting and even eyebrow raising it is not considered evidence by the vast majority of the scientific community because the cited evidence amounts to little more than very timely circumstantial or anecdotal evidence. That’s what’s known as “junk science” among true investigators that depend on large cohort (group) double blind studies.
A lot of negative charges have been leveled at Aspartame but there’s little or no real scientific evidence to back any of it up. Here are some examples of what can be found on the internet
- NutraSweet® killed my mother and has killed and/or wounded millions of innocent people in the US and abroad.
- Aspartame converts to formaldehyde in vivo in the bodies of laboratory rats.
- ARTIFICIAL SWEETENER, ASPARTAME, (EQUAL, NUTRASWEET) LINKED TO BREAST CANCER AND GULF WAR SYNDROME.
- Did O.J. Simpson have a reaction to Aspartame that led to the deaths of Nicole Simpson and Ron Goldman?
- The FDA, the International Food Information Council (IFIC), public Voice and others are scam non-profit organizations and pawns of the Nutra-Sweet Company.
- After more than twenty years of aspartame use the number of its victims is rapidly piling up and people are figuring out for themselves that aspartame is at the root of their health problems. Patients are teaching their doctors about this nutritional peril, and are healing themselves with little to no support from traditional medicine.
- Donald Rumsfeld disregarded safety issues and used his political muscle to get Aspartame approved.
Much of the criticism of Aspartame is absolute nonsense but some is based on a study conducted in 2005 by the European Ramazzini Foundation, which tracked the health of aspartame-fed rats for their entire natural lives.  The study linked aspartame consumption with an increased lifetime cancer risk. But the U.S. Food and Drug Administration (FDA) says aspartame is safe in doses of 50mg per kilogram of body weight. That means that a 165 pound adult could safely drink 21 diet sodas a day. The Ramazzani study fed Aspartame to rats in extremely high doses that ranged from 8 to over 2000 sodas a day…2000? Do you know anyone who even drinks 8?
The study linked aspartame consumption with an increased lifetime cancer risk. But the U.S. Food and Drug Administration (FDA) says aspartame is safe in doses of 50mg per kilogram of body weight. That means that a 165 pound adult could safely drink 21 diet sodas a day. The Ramazzani study fed Aspartame to rats in extremely high doses that ranged from 8 to over 2000 sodas a day…2000? Do you know anyone who even drinks 8?
To be fair, let’s look at a couple of other studies. Researchers from the University of Miami and Columbia University found that people who drink diet soda every day have a 43 percent higher risk of experiencing a vascular event over a 10-year period, compared with people who didn’t drink soda. Plus, this association held true even after taking into account known stroke and heart risk factors like diabetes and high blood pressure. And in a study published in the American Journal of Clinical Nutrition, French researchers found an association between Type 2 diabetes and self-reported diet soda consumption. Plus, when comparing the diabetes risk of drinkers of diet with drinkers of regular sodas, researchers found that diet drinkers had the higher diabetes risk.
But again, these studies are observational. It’s unknown if the diet soda is actually causing these conditions, or if people who are already at high risk for a heart attack, stroke and Type 2 diabetes tend to drink diet soda in an effort to lead a healthier lifestyle. Research on diabetes and diet soda consumption has been mixed so far; a review of studies from Harvard researchers published in 2011 showed no link between diet soda consumption and increased Type 2 diabetes risk.
While nothing can be considered 100 percent safe, aspartame has undergone extensive testing. With the exception of a few very mild side effects, aspartame appears to be quite safe. Those individuals, who experience problems after consuming aspartame, should eliminate foods and beverages that contain this sweetener from their diet.
The previous paragraphs pointing to the safety of Aspartame are supported by this evidence.
http://www.livescience.com/36257-aspartame-health-effects-artificial-sweetener.html
In 1965, James M. Schlatter, a chemist at G.D. Searle and Company, accidentally contaminated the tip of his index finger with an unassuming white powder. Later that day, a page in the book he was reading got stuck. He licked his fingertip to turn the page, and inadvertently gave birth to an entire industry, as well as a seemingly eternal controversy.
The substance on Schlatter’s finger, 200 times sweeter than sugar, was aspartame, the artificial sweetener known today by the brand names NutraSweet, Equal and Spoonful. Almost 50 years after Schlatter discovered aspartame’s incredible sweetness, disagreement still exists among scientists about whether it’s safe for human consumption.
 In essence, aspartame consists of two amino acids with an extra carbon atom stuck on one end. Aspartame breaks down completely into these three components in the small intestine, and they make their way separately into the blood.
In essence, aspartame consists of two amino acids with an extra carbon atom stuck on one end. Aspartame breaks down completely into these three components in the small intestine, and they make their way separately into the blood.
One of aspartame’s two amino acids, aspartic acid, is non-essential, which means the body can manufacture it from other raw materials. Aspartic acid is also a neurotransmitter, which has led to speculation that aspartame consumption affects normal brain processes, possibly causing headaches, migraines, or worse. Almost all dietary protein contains aspartic acid, however, and the aspartic acid found in artificially sweetened foods and drinks pales in terms of quantity to the amount gained through a normal diet.
However, phenylalanine, the other amino acid in aspartame, is another story – but only for the small subset of the population. Phenylalanine is an essential amino acid, which means the body can only acquire it through the diet. For sufferers of the disease phenylketonuria, ingesting this amino acid leads to a dangerous buildup of phenylalanine that can damage the brain.
Although the amino acids comprising the bulk of aspartame are harmless for most people, the scientific jury is still deliberating about that extra carbon atom tacked on the end of the molecule. When an aspartame molecule breaks apart in the small intestine, this carbon disengages from the amino acids and forms a single molecule of methanol.
Methanol, also known as wood alcohol, is found in antifreeze and rocket fuel, among many other applications. Methanol’s effect on the body is similar in some ways to that of ethanol (the alcohol found in wine and beer), but unlike ethanol, the body deals with methanol by transforming it into waste products that include formaldehyde, a carcinogen that morticians use as embalming fluid.
If aspartame delivers methanol to your bloodstream, it would seem like a no-brainer to avoid the sweetener at all costs, but there’s a confounding factor: methanol is also found in all sorts of harmless foods, especially fruits and vegetables, in quantities comparable to foods that contain aspartame. In fact, aspartame-flavored soda contains less than half the methanol found in the same volume of many fruit juices.
This is where the dialogue gets contentious. To some researchers, it’s clear that methanol is harmless in the small quantities derived from aspartame-containing foods. However, a study conducted in 2005 by the European Ramazzini Foundation, which tracked the health of aspartame-fed rats for their entire natural lives, linked aspartame consumption with an increased lifetime cancer risk.
Some researchers, as well as the U.S. Food and Drug Administration, found fault with the study’s methods, while other scientists rushed to defend it, saying that at the very least, aspartame requires continued examination. At the heart of the debate is the fact that in rats, as in humans, a large percentage of individuals will succumb to cancer in very old age. It’s difficult for scientists to say whether cancer in a very old rat was caused by lifetime ingestion of a substance such as aspartame, or whether the cancer would have occurred naturally.
It is also important to point out that rats are not humans and often what occurs in a rat study doesn’t happen if later repeated in a human study. The physical makeup of a rat is simply not the same as a human and while information gained from the animals may be helpful it is never regarded as proof of what will happen in people.
As the debate surrounding the long-term safety of aspartame persists, it’s important to consider the sweetener not in terms of its absolute safety, but whether it’s healthier than the alternative: sugar. Given rising levels of diabetes and obesity in the United States, it’s possible that for some people, a zero-calorie sugar alternative that carries some risks may still be a healthier choice than sugar. And in the meantime, new artificial sweeteners such as sucralose are flooding the market, which may or may not carry their own health risks.
There is one sure-fire healthy alternative to both artificial sweeteners and sugar, of course. don’t drink them. Try a glass of ice water instead or perhaps unsweetened coffee or tea.
The European Food Safety Authority (EFSA) recently reviewed that 2005 Ramazzini Foundation study cited earlier. They found multiple significant flaws and concluded:
“The data on total malignant tumours do not provide evidence of a carcinogenic potential of aspartame.”
As with any health issue it is unwise to adopt the results of one lab or one study. When there have been hundreds of studies on a question, the cherry pickers will always have a lot to choose from. That is why systematic reviews are necessary,
Let me offer one more piece of evidence as to the safety of Aspartame. http://www.sciencebasedmedicine.org/aspartame-truth-vs-fiction/ By Steven Novella September 15, 2010
If you believe everything you read on the internet, then is seems that a chemical found in thousands of products is causing an epidemic of severe neurological and systemic diseases, like multiple sclerosis and lupus. The  FDA, the companies that make the product, and the “medical industrial complex” all know about the dangers of this chemical but are hiding the truth from the public in order to protect corporate profits and avoid the pesky paper work that would accompany the truth being revealed. The only glimmer of hope is a dedicated band of bloggers and anonymous e-mail chain letter authors who aren’t afraid to speak the truth. Armed with the latest anecdotal evidence, unverified speculation, and scientifically implausible claims, they have been tirelessly ranting about the evils of this chemical for years. Undeterred by the countless published studies manufactured by the food cartel that show this chemical is safe, they continue to protect the public by spreading baseless fear and hysteria.
FDA, the companies that make the product, and the “medical industrial complex” all know about the dangers of this chemical but are hiding the truth from the public in order to protect corporate profits and avoid the pesky paper work that would accompany the truth being revealed. The only glimmer of hope is a dedicated band of bloggers and anonymous e-mail chain letter authors who aren’t afraid to speak the truth. Armed with the latest anecdotal evidence, unverified speculation, and scientifically implausible claims, they have been tirelessly ranting about the evils of this chemical for years. Undeterred by the countless published studies manufactured by the food cartel that show this chemical is safe, they continue to protect the public by spreading baseless fear and hysteria.
Hopefully, you don’t believe everything you read on the internet, and you don’t get your science news from e-mail SPAM, where the above scenario is a common theme. While there are many manifestations of this type of urban legend, I am speaking specifically about aspartame – an artificial sweetener used since the early 1980s. The notion that aspartame is unsafe has been circulating almost since it first appeared, and like rumors and misinformation have a tendency to do, fears surrounding aspartame have taken on a life of their own.
I am frequently asked my opinion about the safety of aspartame. Nutritionists often council to avoid the sweetener, citing unverified claims that it is unsafe. I was recently sent a chain letter warning that aspartame causes MS (which of course can be cured by simply avoiding aspartame), and![]() Snopes informs me that this particular letter first appeared in 1998.
Snopes informs me that this particular letter first appeared in 1998.
There are also hundreds of websites dedicated to smearing this much abused food additive. One site, run by Dr. Janet Starr Hull (she has a doctorate in Nutrition), responds to the latest report of aspartame’s safety by writing:
I will never accept the news of aspartame safety. I think it is a “business” decision to discredit/discount the research results that aspartame DOES cause cancer, major nerve disorders, birth defects, and brain imbalances. Think about it – can you imagine the chaos that will occur when the truth of aspartame dangers is accredited. The FDA has known about the dangers, the corporations have known about the dangers, and the medical community (if it is really worth anything) has known about the dangers.
The statement that “nothing will ever convince me” is a huge red flag that someone is defending an ideological position, one immune to evidence or reason. Admittedly, in context it could be a clumsy statement that something is very unlikely. It would be very difficult to convince me that the earth is flat – I’m really saying that the existence evidence is overwhelming that the earth is not flat. But that is not what Dr. Hull is saying. She is specifically saying that she will dismiss any evidence that is contrary to her belief that aspartame is not safe on the a-priori basis that such disconfirming evidence is part of a vast conspiracy.
Of course, Dr. Hull also sells an aspartame detox kit, which might lead a cynical person to conclude that she cares more about selling alternative health products and stoking her sales with some unreasonable fear than about scientific evidence.
What evidence does she have for such a conspiracy? The argument from final consequences logical fallacy – big industry wouldn’t want it. It’s also not very plausible. Products get pulled from the market all the time when new evidence suggests they are not safe. Also, the final safety net for the consumer is legal liability. Class action law suits have bankrupted companies, even when the underlying claims were false. Imagine if they were true. Look how much the tobacco industry has had to fork over.
Now I am not arguing that corporations are all good corporate citizens or wouldn’t dream of sweeping some inconvenient evidence under the carpet. But I am saying that a decades long conspiracy among industry, federal regulatory agencies, the medical community, and multiple research institutions and individual researchers – all under the nose of the press and lawyers looking for big class-action suits – is implausible in the extreme. I am also arguing that we should fairly assess all the evidence, not just cherry pick the evidence we like and dismiss the rest out of hand.
What does the evidence say about aspartame? A recent published review of all available evidence, including hundreds of studies, concluded:
The studies provide no evidence to support an association between aspartame and cancer in any tissue. The weight of existing evidence is that aspartame is safe at current levels of consumption as a nonnutritive sweetener.
Multiple reviews, going back to 1985, conclude the same thing. Since this latest review there have been more studies, in various countries (how big is this conspiracy?), showing no link between aspartame and brain cancer, and a lack of correlation between artificial sweeteners and gastric, pancreatic, and endometrial cancers.
Like all such research, there is noise in the data (but no apparent signal). There is no pattern of evidence to suggest that aspartame causes cancer, autoimmune disease, neurological disease, diabetes, or anything else its critics claim. What legitimate scientific controversy there is comes from the animal data, mostly in rats. Here the evidence for a carcinogenic or genotoxic (causing changes in the DNA) effect of aspartame is mixed and requires careful review. Some effects, such as a dose-dependent effect on renal tumors, are specific to rats and do not translate to humans. Other studies are plagued by significant flaws, such as properly calculating doses (a big issue when trying to extrapolate doses from rats to humans). And still others show flat effects without a dose response curve, suggesting that a confounding factor, and not aspartame, is responsible for any observed increase in tumors.
For example,
Animals studies are problematic and have produced mixed results, but no clear evidence of a neoplastic risk.
A separate question is whether or not aspartame causes headaches in some people. While there is not a lot of specific data on this, there are case reports of aspartame triggering migraines in susceptible people. Migraineurs frequently have multiple food triggers, and there is a long list of foods known to be potential migraine triggers. This is not evidence for toxicity. So while evidence is lacking to demonstrate aspartame is a headache trigger, this is not implausible and not particularly worrisome. What I recommend to patients with frequent headaches is to keep a headache diary, rather than trusting to memory (and confirmation bias) to detect real associations. If there is a clear pattern between a potential trigger and headaches, then avoid that trigger.
Yet another distinct question about artificial sweeteners (not just aspartame) is whether or not they contribute to obesity by interfering with brain’s association between sweetness and calories. The theory is that using zero-calorie sweeteners dissociates the sensation of sweetness from caloric intake, so that sweetness will cause less satiety, leading to increases in overall sugar and calorie consumption.
The question of aspartame and weight control is a complex one, and can be approached from many research angles. Here is a recent review of research. At present the question is very much unsettled. It seems that there is no significant metabolic and no demonstrated neuronal effect from artificial sweeteners. However, people who knowingly consume diet drinks do tend to overcompensate by consuming greater calories overall. While studies of substituting aspartame for sugar in a blinded fashion show that calories are reduced, contributing to weight loss.
By my reading, the current summary of available research is that consuming calories in drinks contributes to weight gain and obesity, substituting calorie-free drinks (whether water or diet drinks containing artificial sweeteners) does help reduce caloric intake and aid in weight control, but there is a tendency to overcompensate by increasing other caloric intake. Therefore it seems reasonable to use artificial sweeteners to reduce caloric intake from drinks, but to be careful to control overall caloric intake (so no, putting aspartame in your coffee does not mean you can eat the cheesecake).
Conclusion
Aspartame is a highly studied food additive with decades of research showing that it is safe for human consumption. As expected, the research is complex making it possible to cherry pick and misinterpret individual studies in order to fear monger. But the totality of research, reviewed by many independent agencies and expert panels, supports the safety of aspartame.
A conspiracy to hide the risks of aspartame, however, remains a popular internet urban legend that will likely not disappear anytime soon.
Finally…this report from National Public Radio. http://www.npr.org/blogs/thesalt/2012/10/24/163559533/aspartame-and-cancer-risk-new-study-is-too-weak-to-defend
Data Linking Aspartame To Cancer Risk Are Too Weak To Defend, Hospital Says
October 24, 2012 5:38 PM
Aspartame is a sugar substitute found in many popular foods, including diet sodas.
By Maggie Starbard NPR
We almost brought you news today about a study that appeared to raise some troubling questions about aspartame, the popular sugar substitute  found in many common foods like diet soda. Note the key word — almost.
found in many common foods like diet soda. Note the key word — almost.
A study due to be published at 3 p.m. Wednesday in the American Journal of Clinical Nutrition and released to reporters earlier in the week under embargo found some correlation between drinking diet soda and an increased risk of leukemia and Non-Hodgkin’s lymphoma, as well as a few other rare blood-related cancers.
But at 2:24 p.m. — about a half-hour before the paper was to publish — we and many other news outlets who had been working on the story got an email from the senior vice president of communications at Brigham and Women’s Hospital.
“It has come to our attention that the scientific leaders at Brigham and Women’s Hospital did not have an opportunity, prior to today, to review the findings of the paper,” Erin McDonough wrote in an email to us. “Upon review of the findings, the consensus of our scientific leaders is that the data is weak, and that BWH Media Relations was premature in the promotion of this work. We apologize for the time you have invested in this story.”
Now, the paper still got , although the editor of the journal, , told us that the reviewers pushed back during the editing process. They wanted to make sure “that the conclusion made it clear that chance was a plausible explanation of the findings,” he says. “The journal tried to ensure that the caveats were adequately presented.”
A co-author of the paper, Harvard’s , who sits on the of the ACJN, told us earlier today by email that “I do think this finding is strong enough to justify further study on aspartame and cancer risk.”
However, it seems as if senior scientists at Brigham and Women’s Hospital decided that the data weren’t ready for prime time. And all along, in the course of our reporting, the researchers we interviewed (who were not connected with the paper) had raised cautions.
“The results are really not that strong,” of the National Cancer Institute told us yesterday.
And from of MD Anderson Cancer Center: “I’m not convinced that this paper shows a relationship between blood-related cancers and drinking diet soda.”
of the American Cancer Society had pointed to inconsistent findings. For instance, the increased risk in Non-Hodgkin’s lymphoma was found only in men, not women. And regular, sugar-sweetened soda also seemed to lead to a similar increased risk of cancer.
And statistically, some of the findings teetered on the edge of significance.
The paper’s lead researcher, of Brigham and Women’s Hospital and Harvard Medical School, acknowledged to us yesterday that her manuscript had been turned down for publication by many other journals, including the Journal of the National Cancer Institute, the Journal of the American Medical Association, The Lancet and the British Medical Journal.
So why were journalists even covering the paper? Well, most of the experts we interviewed agreed with Willett that — despite the limitations — the findings were significant enough to justify further research.
As we earlier this week, Americans drink a lot of diet soda, and there’s some evidence that it can help maintain weight.
So we get it. Any evidence that there’s a potential health concern with something as popular and ubiquitous as diet soda has to be pretty solid.
As journalists at NBC , “the situation is a great example of why the public often finds science confusing and frustrating.”
We’ll keep you posted as we learn more.
Well, there you have it. The Benefit of my research on the subject of Aspartame. I think we should all avoid sugar and its substitutes but that’s up to each of you to decide. If you insist on using aspartame or the products that include it do it in moderation. That’s good advice for almost anything you consume…do it in moderation.
 Bob Aronson of Bob’s Newheart is a 2007 heart transplant recipient, the founder of Facebook’s nearly 3,000 member Organ Transplant Initiative and the author of most of these donation/transplantation blogs.
Bob Aronson of Bob’s Newheart is a 2007 heart transplant recipient, the founder of Facebook’s nearly 3,000 member Organ Transplant Initiative and the author of most of these donation/transplantation blogs.
You may comment in the space provided or email your thoughts to me at bob@baronson.org. And – please spread the word about the immediate need for more organ donors. There is nothing you can do that is of greater importance. If you convince one person to be an organ and tissue donor you may save or positively affect over 60 lives. Some of those lives may be people you know and love.
Please view our new music video “Dawn Anita The Gift of Life” on YouTube https://www.youtube.com/watch?v=eYFFJoHJwHs. This video is free to anyone who wants to use it and no permission is needed.
If you want to spread the word personally about organ donation, we have another PowerPoint slide show for your use free and without permission. Just email me bob@baronson.org and ask for a copy of “Life, Pass it on.“ This is NOT a stand-alone show; it needs a presenter but is professionally produced and factually sound. If you decide to use the show I will send you a free copy of my e-book, “How to Get a Standing “O” that will help you with presentation skills.
Also…there is more information on this blog site about other donation/transplantation issues. Additionally we would love to have you join our Facebook group, Organ Transplant Initiative The more members we get the greater our clout with decision makers.
Stop Eating What’s Killing You! Great Tasting Food Ideas ~ Less Salt and Sugar
By Bob Aronson

Tired of paying for expensive prescription drugs? Sick to death of the high cost of health care? Frustrated with trying to find affordable insurance that actually covers something? Upset because your employer doesn’t offer insurance?
There is a solution…at least a partial solution and that is to take better care of yourself. Mos of our ills are brought on by our lifestyles by the fact that we eat wrong, don’t exercise and abuse our bodies in a million other ways.
Sugar is not healthy. We know that products loaded with sugar are not healthy and we know that foods with saturated fat are not healthy but we eat them anyway. Why is that? Simple answer. They are fast, easy and they really taste good!

The rap on eating healthy is that really healthy stuff usually doesn’t taste very good. Let’s face it, when you take away the salt, fat and sugar food can be pretty bland. The taste buds send frantic messages to the brain pleading for relief, “C’mon…just a little more salt…blechhh this tastes awful.”
What we are really saying is that compared to what we have been eating a healthier diet has no taste at all. The fact is the taste of healthier foods is quite distinct, it’s just that all that salt, sugar and fat have masked it and your taste buds need some retraining.
Years ago when I was first told that I might need a heart transplant some day and that I had to change my diet if I wanted to live long enough to get one I was advised to severely limit the amount of sodium in my diet. At the most I could have 2,000 milligrams (2 grams} of sodium per day. When you consider that a Papa John’s 14 inch Pepperoni Pizza with original crust has 825 mgs of sodium per slice and you rarely eat just one slice, you could easily consume your entire day’s allocation of sodium at one sitting.
I used to love salt and still do but I have learned to restrain myself. I was one of those guys who salted everything even before I tasted it. I would put salt on a sausage, pepperoni and extra cheese pizza as soon as it arrived at the table. I used to put salt in my beer, too, so when I could no longer do that all my favorite foods suddenly tasted terrible. That’s when a huge neon sign appeared over my head flashing the message, “It wasn’t the pIzza you loved, it was the salt!” Wanting to live a little longer I took the advice of my physicians and I cut salt intake in two ways. First I did not add salt to anything. Secondly I began to study the labels on food in the grocery store.
Wanting to live a little longer I took the advice of my physicians and I cut salt intake in two ways. First I did not add salt to anything. Secondly I began to study the labels on food in the grocery store.  Limiting yourself to 2 grams of sodium a day is very difficult and for a while you will not like what you are eating – it tastes bland. your taste buds will scream for salt as loudly as a heroin addicts brain screams for narcotic relief. Slowly, though, your taste buds recover from a decades long carpet bombing of sodium … and the real taste of food begins to emerge. Green beans have a distinct taste; pasta, has a taste of its own; even a good lean steak has a unique taste when you remove the salt and the steak sauce and the ketchup, too…sorry.
Limiting yourself to 2 grams of sodium a day is very difficult and for a while you will not like what you are eating – it tastes bland. your taste buds will scream for salt as loudly as a heroin addicts brain screams for narcotic relief. Slowly, though, your taste buds recover from a decades long carpet bombing of sodium … and the real taste of food begins to emerge. Green beans have a distinct taste; pasta, has a taste of its own; even a good lean steak has a unique taste when you remove the salt and the steak sauce and the ketchup, too…sorry.
Don’t get me wrong, we need salt to keep our bodies functioning properly but, we don’t need much (e.g., between about 180 mg and 500 mg per day).
According to the U.S. Centers for Disease Control (CDC) The Institute of Medicine recommends 1500 mg of sodium per day as the Adequate Intake level for most Americans and advises everyone to limit sodium intake to less than 2300 mg per day, the Tolerable Upper Limit.
Once you overcome the taste issue you will begin to enjoy food again. But you don’t have to do it cold turkey. There are plenty of good substitutes for salt that add a dash of extra flavor without being a threat to your health. For example
Here’s some advice from the famed Cleveland Clinic
http://my.clevelandclinic.org/heart/prevention/askdietician/ask1_02.aspx
Ideally, the best way to go is completely “Salt Free.” Instead of mimicking the taste of sodium with salt substitutes, start experimenting with other more flavorful herbs and spices to add zest to your meals. Try fresh garlic or garlic powder, lemon juice, flavored vinegar, salt-free herb blends, cumin, nutmeg, cinnamon, fresh ground pepper, tarragon, oregano and many others to unleash the powerful flavors these salt-free herbs and spices have to offer.
Remember that a 2 gram sodium restriction includes the total sodium in your day – this includes the foods that you eat, not just the seasoning that you add. Be cautious of nutrition labels and keep foods under 140 mg or less which is considered a “low sodium food”.
Another reason for our poor eating habits is lack of time. Everyone seems rushed with no time to be considering sodium, saturated fat or sugar content. We just need something fast – but fast doesn’t have to mean unhealthy.
“Sometimes cooking takes a lot of time in our life, but we got some good news for you. We gathered an excellent list of cooking recipes which are easy to prepare. There are categories of receipts like Breakfast, Salad Entrees, Soups, Fish, Chicken and Turkey, Lean Meat, Vegetarian Entrees, Side Salad/Dressings, Side Vegetables, and Desserts. All easy healthy foods so you don’t even need to think about what to cook tonight!”
[Update: Try this lifehack article for an updated List of 100 healthy recipes that you can learn in 15 minutes]
I edited the list so if you want the complete story click on this link: http://www.lifehack.org/articles/lifehack/over-100-quick-and-easy-healthy-foods.html
Or…for great and flavorful healthy food ideas go directly to Recipesia dot com. http://www.recipesia.com/
Breakfast
Mission Fritada With Wine Syrup
Scrambled Eggs With Shrimp And Sherry
Salad Entrees
Soups
Sweet Red Pepper And Crab Bisque
Fish
Chicken and Turkey
Chicken With White Wine And Mushrooms
Lean Meat
Vegetarian Entrees
Deep Fried Masa Turnovers With Cheese
Green Chile Avocado Enchiladas
Black Eyed Pea And Vegetable Stew
Bulghur Wheat “sausage” Patties
Side Salad/Dressings
Creamy Romaine Salad – non-dairy
Side Vegetables
Calabacitas – Mexican flavored vegetable side dish
Healthy Mashed Sweet Potatoes – no dairy
Desserts
Bailey’s Chocolate Mousse Cheesecake
Bailey’s Irish Cream Cheesecake
Baklava Cheesecake
Got some ideas for healthier living? We’d like to hear them. Please add your comments here or write to me directly bob@baronson.org if you have a blog idea or if you’d like to submit a guest blog. Stay tuned for more on living healthy. One way of solving the transplantable organ shortage is by reducing the demand. By living healthy you do just that.
-0-
 Bob Aronson of Bob’s Newheart is a 2007 heart transplant recipient, the founder of Facebook’s nearly 3,000 member Organ Transplant Initiative and the author of most of these donation/transplantation blogs.
Bob Aronson of Bob’s Newheart is a 2007 heart transplant recipient, the founder of Facebook’s nearly 3,000 member Organ Transplant Initiative and the author of most of these donation/transplantation blogs.
You may comment in the space provided or email your thoughts to me at bob@baronson.org. And – please spread the word about the immediate need for more organ donors. There is nothing you can do that is of greater importance. If you convince one person to be an organ and tissue donor you may save or positively affect over 60 lives. Some of those lives may be people you know and love.
Please view our new music video “Dawn Anita The Gift of Life” on YouTube https://www.youtube.com/watch?v=eYFFJoHJwHs. This video is free to anyone who wants to use it and no permission is needed.
If you want to spread the word personally about organ donation, we have another PowerPoint slide show for your use free and without permission. Just go to http://www.organti.org and click on “Life Pass It On” on the left side of the screen and then just follow the directions. This is NOT a stand-alone show; it needs a presenter but is professionally produced and factually sound. If you decide to use the show I will send you a free copy of my e-book, “How to Get a Standing “O” that will help you with presentation skills. Just write to bob@baronson.org and usually you will get a copy the same day.
Also…there is more information on this blog site about other donation/transplantation issues. Additionally we would love to have you join our Facebook group, Organ Transplant Initiative The more members we get the greater our clout with decision makers.
En Espanol
Puede comentar en el espacio proporcionado o por correo electrónico sus pensamientos a mí en bob@baronson.org. Y – por favor, difundir la palabra acerca de la necesidad inmediata de más donantes de órganos. No hay nada que puedas hacer lo que es de mayor importancia. Si usted convence a una persona de ser donante de órganos y tejidos puede salvar o afectar positivamente a más de 60 vidas. Algunas de esas vidas pueden ser personas que conoces y amas.
Por favor, consulte nuestro nuevo video musical “Dawn Anita The Gift of Life” en https://www.youtube.com/watch?v=eYFFJoHJwHs YouTube. Este video es libre para cualquier persona que quiera usarlo y no se necesita permiso.
Si quieres correr la voz acerca de la donación de órganos personalmente, tenemos otra presentación de PowerPoint para su uso libre y sin permiso. Sólo tienes que ir a http://www.organti.org y haga clic en “Life Pass It On” en el lado izquierdo de la pantalla y luego sólo tienes que seguir las instrucciones. Esto no es un espectáculo independiente, sino que necesita un presentador pero es profesionalmente producida y sonido hechos. Si usted decide usar el programa le enviaré una copia gratuita de mi libro electrónico, “Cómo obtener un pie” O “que le ayudará con habilidades de presentación. Sólo tiene que escribir a bob@baronson.org y por lo general usted recibirá una copia del mismo día.
Además … hay más información sobre este sitio de blogs sobre otros donación / trasplante temas. Además nos encantaría que te unas a nuestro grupo de Facebook, la Iniciativa de Trasplante de Órganos Cuantos más miembros que obtenemos mayor será nuestra influencia con los tomadores de decisiones.
50 Ways to Add Years to Your Life (From Men’s Health)
 From Men’s Health Magazine
From Men’s Health Magazine
50 Ways to add years to your life
http://www.menshealth.com/health/50-ways-add-years-your-life?onepage=1
Overview
We’ve been told that the only sure things are death and taxes. But just as creative accountants have helped many triumph over their 1040s, we can help outrun the reaper. Maybe it’s a game you can’t ultimately win. But by following these 50 tips, you sure as hell can send it into overtime (while published in a men`s magazine these tips are not gender exclusive. . They work regardless of sexual persuasion ….. Bob Aronson 🙂
Drink 5 8-Ounce Glasses of Water a Day
Scientists at Loma Linda University found that men who drank this amount of H2O were 54 percent less likely to suffer a fatal heart attack than those who drank two glasses or less every day.
Take a Laugh Break
- Watching 15 minutes of funny video can improve bloodflow to your heart by 50 percent, report researchers at the University of Maryland. “This may reduce blood-clot formation, cholesterol deposition, and inflammation,” says study author Michael Miller, M.D

Don’t Go to Work Sick
- Over a 3-year period, men who clocked in despite feeling under the weather had double the heart-attack risk of guys who stayed in bed, according to a U.K. study.
Put Out the Fire in Your Chest
- Untreated heartburn can lead to a heart attack, according to a study in the International Journal of Cardiology. Scientists discovered that as acid levels in the esophagus rise, the incidence of blocked bloodflow to the heart also rises by 20 percent. A natural remedy: Analyze your diet. Don’t make a habit of drinking wine, juice, or carbonated beverages, all of which are highly acidic and may trigger heartburn, say South Carolina researchers.
Indulge Your Chocolate Craving
- In a 15-year study, Dutch scientists determined that men who ate just 4 grams of cocoa a day had half the risk of dying from heart disease than those who ate less. That’s the equivalent of two 25-calorie Hershey’s Kisses—an amount that can fit into any diet.
Say No to Froot Loops
- In a review of 53 studies, Australian researchers found that regularly eating cereal made from refined grains raises insulin and C-reactive protein, and lowers good cholesterol—all factors that boost your odds of developing heart disease. A better choice for your morning bowl: Post Shredded Wheat cereal, which is made from 100 percent whole grains and contains no sugar.
Take a Magnesium Supplement
- Over an 18-year period, French researchers determined that men with the highest blood levels of magnesium are 40 percent less likely to die of any cause than those with the lowest levels. Magnesium can make multivitamins too bulky, so add a 250 milligram (mg) pill from iherb.com or GNC to your daily regimen.
Burn 1,100 Calories a Week
- Duke University scientists discovered that this amount of exercise prevents the accumulation of visceral adipose tissue—the dangerous belly fat that causes arterial inflammation and hypertension. Falling short? Join a league: A recent British Medical Journal study reported that people who exercised in groups boosted their average calorie burn by 500 a week.
Take a Daily Multivitamin
- Researchers at the University of California at Berkeley discovered that this helps prevent the DNA damage that causes cancer. We like Centrum Silver.
Hit the Weights
- University of Michigan scientists found that men who completed three total-body weight workouts a week for 2 months lowered their diastolic blood pressure (the bottom number) by an average of eight points. That’s enough to reduce the risk of stroke by 40 percent and heart attack by 15 percent.
Set a 3-Drink Limit
- Harvard researchers determined that downing more than three drinks in a 24-hour period increases your risk of atrial fibrillation, a condition that may boost your odds of a stroke fivefold during that time. An important note: When the average man pours himself a glass of wine, it’s typically twice the size of a standard drink (4 ounces), report researchers at Duke University.
Plop an Alka-Seltzer . . .
- If you think you’re having a heart attack. It contains 325 milligrams of aspirin, the same as a regular aspirin, and begins fighting blood clots almost 3 minutes faster than a pill, according to a study in Thrombosis Research.
. . . and Call a Ride
- Walk-in patients wait almost twice as long in the E.R. as those who arrive by ambulance, according to a University of New Mexico study.
Treat a Killer Bee Sting
- You may not know if you’re allergic to the venom of a bee, wasp, or hornet until you’ve already been stung. But if you start to experience the symptoms of a life-threatening reaction—hives, wheezing, abdominal cramping—you can save yourself in 3 steps:
- Step 1: Call 911.

Step 2: Take a Benadryl.
Step 3: Lie on your back and elevate your legs while you wait for help, says Steven Kernerman, D.O., an allergist at the Spokane Allergy and Asthma Clinic. An allergic reaction can constrict your blood vessels, and our three-step strategy counteracts that by improving bloodflow to your heart.
Eat Produce at Every Meal
- If you consume more than five servings of fruits and vegetables per day, you have a 26 percent lower risk of stroke than people who eat fewer than three servings, according to a recent U.K. study.
Monitor Your Blood Sugar
- Johns Hopkins University researchers recently determined that people with the highest blood-sugar levels have twice the risk of heart disease as those with the lowest. A warning sign: fasting blood sugar that’s greater than 100 mg per deciliter.
Think Positive
- Purdue scientists discovered that constant worrying shortens your life span by 16 years.
Keep Your Cool
- Men who frequently express anger outwardly are more than twice as likely to have a stroke than guys who control their tempers, according to the journal Stroke. If you have anger-management issues, try fish oil. National Institutes of Health scientists found that hostile, aggressive men often have low blood levels of DHA—one of the main omega-3 fats found in the oil. We like Nordic Naturals Ultimate Omega (nordicnaturals.com). Take 1,000 to 2,000 mg every day.
Dive with a Partner
- This cuts the chance of a shark attack by 50 percent, say Australian scientists. Most shark attacks occur at dawn and dusk, when sharks feed, says Alan Henningsen, a marine biologist and shark researcher at the National Aquarium in Baltimore. You can watch the sky for clues to their location: Seabirds eat the same fish as sharks.
Hit the Shark in Its Eyes or Gills
- These are its most sensitive areas. The snout might work as a target, but this tactic often results in a bitten arm if you are attacked, according to a University of Maryland study.
For God’s Sake, Don’t Pee in the Ocean
- Bodily fluids attract sharks.
Try a Natural Remedy
- According to Israeli scientists, eating one red grapefruit a day lowers LDL (bad) cholesterol by 20 percent, even in people who don’t respond to statins.
Eat Breakfast Within 90 Minutes of Waking
- A University of Massachusetts study found that men who waited longer than that were 50 percent more likely to become obese. And U.K. researchers determined that increases in body mass were directly proportionate to the likelihood of dying of gut cancers—specifically rectal, bladder, colon, and liver.
Vacuum for 30 Minutes
- Doing 150 calories’ worth of chores a day can lower high blood pressure by 13 points, according to Medicine & Science in Sports & Exercise. The reduction lasts only 8 hours, but make it a daily habit and you can lower your BP in the long term. (Helping out more with housework may improve your sex life, too.)

Eat Berries
- The antioxidants in cranberries, blueberries, strawberries, and raspberries have been shown to offer protection from a stroke, keep you mentally sharp as you age, and ward off cancer.
Drownproof Yourself
- If you’re dumped in the water without a life preserver, the key to survival is staying warm and conserving energy. Use the method taught to U.S. Navy pilots: Float facedown in the water with your knees tucked against your chest in the fetal position. (This slows the drop in body temperature.) Exhale bubbles slowly, turning your head to one side only to inhale deeply. Repeat until help arrives.
Sleep on Your Side
- This can halve the number of sleep-apnea-related wakeups you experience during the night. Such interruptions make you up to six times more likely to be involved in an auto accident, due to residual fatigue, according to researchers at University Hospital in Bern, Switzerland. To keep from rolling over onto your back as you sleep, stuff a small, firm neck pillow down the back of your T-shirt before dozing off.
Light a Jasmine-Scented Candle
- Men who did this for just 1 minute before bed fell asleep faster, tossed and turned less, and felt more refreshed in the morning than those who didn’t inhale the aroma, report scientists at Wheeling Jesuit University. That’s important, because insufficient sleep boosts your risk of diabetes, and restless sleep increases your odds of a stroke.
Live Life in a Smoke-Free Zone
- Secondhand smoke, besides boosting your risk of lung cancer, raises your diabetes risk by 40 percent-—nearly the same as smoking does.
Dodge a Deadly Lightning Bolt
- Stay off the toilet during severe thunderstorms. If lightning hits within even 60 feet of your house, it can not only jump through phone and electrical lines but also run through plumbing, according to the National Weather Service.
Put Your iPod on a Mount
- Reaching for an unsecured object as you drive makes you eight times more likely to swerve into a road barrier, according to the Mayo Clinic.
Check Your Smoke Alarms
- The most likely reason a house fire ends in a fatality: no early warning. While just about every U.S. residence has smoke alarms, a Morehouse School of Medicine study revealed that the devices were nonfunctioning in one-third of homes due to dead or absent batteries. If you’ve ever let the juice in any of your detectors dwindle—or removed the battery simply to disable the low-power beep—consider installing at least one DuPont self-charging smoke alarm. It screws into a ceiling light socket and feeds off your home’s electricity.
Sip on Mint Tea
- It contains the powerful antioxidant hesperidin, which reduces the inflammation and oxidative stress associated with diabetes by 52 percent, according to a study at the University of Buffalo. And despite its lack of caffeine, mint tea also increases alertness.
Don’t Jaywalk
- This is particularly good advice if you’ve had too much to drink, because 77 percent of pedestrians killed while crossing the road aren’t at intersections. And 53 percent of those killed at night had blood-alcohol concentrations at or above .08 percent, the legal limit in all 50 states.
Don’t Get Blown to Bits
- Keep bleach, paint stripper, fabric softener, glue, and sidewalk salt away from gas appliances. The chlorine or fluorine in these products breaks down into ionized gas, which can eat holes in the pipes that deliver the fuel for your furnace, range, or dryer. Think you smell fumes? Don’t call for help from inside your house; using your phone could create an electric spark and set off an explosion.
Find Time to Exercise . . .
- Improve your outlook and save your life. Scandinavian researchers have observed that deep depression (and its spinoff, suicide) is often caused by job stress. Here’s how to lower stress, boost your mood, and simultaneously improve your overall health. People who exercise at any intensity for 2 hours a week—an average of about 17 minutes a day—are 61 percent less likely to feel highly stressed than their sedentary counterparts, according to researchers in Denmark.
. . .Then Take It Outside
- British researchers found that people who exercised outdoors reduced their depression by 71 percent, while indoor exercisers’ depression decreased by only 45 percent after their workouts.
Cut Out the Sweet Stuff
- Tufts University researchers found that men on low-sugar diets had lower levels of depression and anxiety than those who consumed all types of carbs. The happier people also limited their total carb intake to 40 percent of total calories.
Douse Your Salad with Oil and Vinegar
- European scientists determined that unheated olive oil reduces cancer risk. As for vinegar, eating it prior to a high-carbohydrate meal (like pasta) slows the absorption of carbs into your bloodstream. This prevents the spikes in blood sugar and insulin that signal your body to store fat.
Add Curry to Vegetables
- Rutgers University scientists discovered that a combination of turmeric (found in curry powder) and phenethyl isothiocyanate (a compound in broccoli, brussels sprouts, and cauliflower) helps fight prostate cancer. The researchers believe that dusting your vegetables just once a week will provide protection.
Be a Career Coach
- A man married to a woman who is upset by her work is 2.7 times more likely to develop heart disease. If your wife won’t find a new job, help her practice her negotiating skills. A Harvard study found that due to anxiety, women don’t initiate money talks at work as often as men do, especially when the boss is male.
Stash an Air Freshener in Your Car
- The strong, spicy smell of cinnamon can help you stay alert as you drive. Researchers at Wheeling Jesuit University found that a whiff increases alertness by 25 percent. Sucking on an Altoid may work, too.
Test Yourself for HIV
Fall on Your Butt
- If you feel yourself losing balance on the stairs, crouch so that your butt hits first, says Robert Nirschl, M.D., a spokesman for the American Academy of Orthopaedic Surgeons. Don’t be afraid to bounce down a few steps—it’ll make a fatal blow less likely.
Design a Colorful Menu
- Colorado State University scientists discovered that men who eat the widest variety of fruits and vegetables gain greater cancer-fighting benefits than those who eat more total servings but choose from a smaller assortment. That’s because the plant chemicals that protect against disease vary between botanical families. Mix it up by choosing one serving from five different color groups: blues and purples, greens, whites, reds, and yellows and oranges.
Take a Noontime Nap
- Breaking up your day with a 30-minute snooze can reduce coronary mortality by 37 percent, report Greek researchers. Why? It reduces stress that can damage your heart. Even a short nap once or twice a week was found to decrease the risk of early death.
Steep Your Tea for at Least 3 Minutes
- Any less than that lowers the number of disease-fighting antioxidants.
Use Watercress in Your Salad
- A study from the American Journal of Clinical Nutrition reveals that eating 3 ounces of watercress every day increases levels of the cancer-fighting anti-oxidants lutein and beta-carotene by 100 and 33 percent, respectively.
Enjoy Your Joe
- Brooklyn College researchers recently discovered that drinking 4 cups of coffee a day lowers your risk of dying of heart disease by 53 percent. If you like Starbucks, choose a Caffe Americano: A grande counts as 4 cups and contains just 15 calories.
Ask for the Heel
- Bread crust has up to eight times more pronyl lysine—an antioxidant that fights cancer—than what’s in the center. Similarly, the skin of produce is loaded with healthy nutrients, too.
Bob Aronson of Bob’s Newheart is a 2007 heart transplant recipient, the founder of Facebook’s nearly 3,000 member Organ Transplant Initiative and the author of most of these donation/transplantation blogs.
You may comment in the space provided or email your thoughts to me at bob@baronson.org. And – please spread the word about the immediate need for more organ donors. There is nothing you can do that is of greater importance. If you convince one person to be an organ and tissue donor you may save or positively affect over 60 lives. Some of those lives may be people you know and love.
Please view our new music video “Dawn Anita The Gift of Life” on YouTube https://www.youtube.com/watch?v=eYFFJoHJwHs. This video is free to anyone who wants to use it and no permission is needed.
If you want to spread the word personally about organ donation, we have another PowerPoint slide show for your use free and without permission. Just go to http://www.organti.org and click on “Life Pass It On” on the left side of the screen and then just follow the directions. This is NOT a stand-alone show; it needs a presenter but is professionally produced and factually sound. If you decide to use the show I will send you a free copy of my e-book, “How to Get a Standing “O” that will help you with presentation skills. Just write to bob@baronson.org and usually you will get a copy the same day.
Also…there is more information on this blog site about other donation/transplantation issues. Additionally we would love to have you join our Facebook group, Organ Transplant Initiative The more members we get the greater our clout with decision makers.
En Espanol
Puede comentar en el espacio proporcionado o por correo electrónico sus pensamientos a mí en bob@baronson.org. Y – por favor, difundir la palabra acerca de la necesidad inmediata de más donantes de órganos. No hay nada que puedas hacer lo que es de mayor importancia. Si usted convence a una persona de ser donante de órganos y tejidos puede salvar o afectar positivamente a más de 60 vidas. Algunas de esas vidas pueden ser personas que conoces y amas.
Por favor, consulte nuestro nuevo video musical “Dawn Anita The Gift of Life” en https://www.youtube.com/watch?v=eYFFJoHJwHs YouTube. Este video es libre para cualquier persona que quiera usarlo y no se necesita permiso.
Si quieres correr la voz acerca de la donación de órganos personalmente, tenemos otra presentación de PowerPoint para su uso libre y sin permiso. Sólo tienes que ir a http://www.organti.org y haga clic en “Life Pass It On” en el lado izquierdo de la pantalla y luego sólo tienes que seguir las instrucciones. Esto no es un espectáculo independiente, sino que necesita un presentador pero es profesionalmente producida y sonido hechos. Si usted decide usar el programa le enviaré una copia gratuita de mi libro electrónico, “Cómo obtener un pie” O “que le ayudará con habilidades de presentación. Sólo tiene que escribir a bob@baronson.org y por lo general usted recibirá una copia del mismo día.
Además … hay más información sobre este sitio de blogs sobre otros donación / trasplante temas. Además nos encantaría que te unas a nuestro grupo de Facebook, la Iniciativa de Trasplante de Órganos Cuantos más miembros que obtenemos mayor será nuestra influencia con los tomadores de decisiones.
We Are Killing Our Own Organs — 30 Worst Foods, 100 Best.
The key to solving the shortage of transplantable organs is to eliminate the demand for them.
“We have met the enemy and he is us,” has become a trite expression but that doesn’t make it any less true. We are our own worst enemies. The numbers are staggering. We are killing ourselves in four ways:
- We drink too much alcohol
- We smoke too much
- We eat too much of the wrong food
Let’s look at he facts.
- 22.5% are current smokers, resulting in significant health problems and associated costs.
- 8.5% of Americans abuse alcohol or are alcohol dependent,.
- Approximately 30.4% of adults in the United States are obese,
The estimated annual medical expenditures associated with alcohol abuse total $26.3 billion. Organs most commonly affected are the lungs, kidneys, pancreas, heart and liver.
Second, smoking. Medical costs caused by cigarette smoking exceed $75 billion a year. According to the Centers for Disease Control in Atlanta, Georgia, Smoking harms nearly every organ of the body and causes many diseases. Cigarette smoking remains the single most-common preventable cause of death in the United States, The adverse health effects from cigarette smoking account for more than 440,000 deaths, or nearly one of every five deaths, each year in the United States.
Finally obesity combined with eating the wrong foods. A good number of these people experience some organ failure. The direct medical costs for obesity have been approximated at $51.6 billion per year. The organs most often affected are the heart, kidneys and pacnreas. http://abcnews.go.com/Health/PictureOfHealth/story?id=4286176&page=1
This blog is about preventing organ failure and one way to do that is to be a little more careful about how much we eat and what we decide to consume. There are two lists here, 1) the worst foods and 2) the best foods.
Top 30 Worst Foods in America (from Food Matters
Note from Bob’s Newheart. While Food Matters lists 30 I am only listing ten. You can click on their link for the rest of the story)
Today’s food marketers have loaded many of their offerings with so much fat, sugar, and sodium that eating any of the foods in this article on a daily basis could destroy all your hard work and best intentions of eating healthy. Beware! This list is brought to you by Eat This Not That and Men’s Health. http://foodmatters.tv/articles-1/the-30-worst-foods-in-america-beware
1. Worst Meal in America
Carl’s Jr. Six Dollar Guacamole Bacon Burger with Medium Natural Cut Fries and 32-oz Coke
1,810 calories – 92 g fat (29.5 g saturated, 2 g trans) – 3,450 mg sodium
Of all the gut-growing, heart-threatening, life-shortening burgers in the drive-thru world, there is none whose damage to your general well-being is as potentially catastrophic as this. A bit of perspective is in order: This meal has the caloric equivalent of 9 Krispy Kreme Original Glazed doughnuts, the saturated fat equivalent of 30 strips of bacon, and the salt equivalent of 10 large orders of McDonald’s French fries!
2. Worst Drink
Baskin-Robbins Large Chocolate Oreo Shake
2,600 calories – 135 g fat (59 g saturated, 2.5 g trans) – 1,700 mg sodium – 263 g sugars
We didn’t think anything could be worse than Baskin-Robbins’ 2008 bombshell, the Heath Bar Shake. After all, it had more sugar (266 grams) than 20 bowls of Froot Loops, more calories (2,310) than 11 actual Heath Bars, and more ingredients (73) than you’ll find in most chemistry sets. Yet the folks at Baskin-Robbins have shown that when it comes to making America fat, they’re always up to the challenge. The large Chocolate Oreo Shake is soiled with more than a day’s worth of calories and 3 days’ worth of saturated fat. Worst of all, it takes less than 10 minutes to sip through a straw.
3. Worst Ribs
Outback Steakhouse Baby Back Ribs
2,580 calories
Let’s be honest: Ribs are rarely served alone on a plate. When you add a sweet potato and Outback’s Classic Wedge Salad, this meal is a 3,460-calorie blowout. (Consider that it takes only 3,500 calories to add a pound of fat to your body. Better plan for a very, very long “walkabout” when this meal is over!)
4. Worst Pizza
Uno Chicago Grill Classic Deep Dish Individual Pizza
2,310 calories – 165 g fat (54 g saturated) – 4,920 mg sodium – 120 g carbs
The problem with deep dish pizza (which Uno’s knows a thing or two about, since they invented it back in 1943) is not just the extra empty calories and carbs from the crust, it’s that the thick doughy base provides the structural integrity to house extra heaps of cheese, sauce, and greasy toppings. The result is an individual pizza with more calories than you should eat in a day and more sodium than you would find in 27 small bags of Lays Potato Chips. Oh, did we mention it has nearly 3 days’ worth of saturated fat, too? The key to success at Uno’s lies in their flatbread pizza.
5. Worst Mexican Dish
Chili’s Fajita Quesadillas Beef with Rice and Beans, 4 Flour Tortillas, and Condiments
2,240 calories – 92 g fat (43.5 g saturated) – 6,390 mg sodium – 253 g carbs
Since when has it ever been a smart idea to combine 2 already calorie- and sodium-packed dishes into one monstrous meal? This confounding creation delivers nearly a dozen Krispy Kreme original glazed doughnuts worth of calories, the sodium equivalent of 194 saltine crackers, and the saturated fat equivalent of 44 strips of bacon. Check please.
6. Worst Seafood Dish
Romano’s Macaroni Grill Parmesan Crusted Sole
2,190 calories – 141 g fat (58 g saturated) – 2,980 mg sodium – 145 g carbs
Fish is normally a safe bet, but this entrée proves that it’s all in the preparation. If you fry said fish in a shell of cheese, be prepared to pay the consequences. Here that means meeting your daily calorie, fat, saturated fat, and sodium intake in one sitting.
7. Worst Chinese Dish
P.F. Chang’s Combo Lo Mein
1,968 calories – 96 g fat (12 g saturated) – 5,860 mg sodium
Lo mein is normally looked at as a side dish, a harmless pile of noodles to pad your plate of orange chicken or broccoli beef. This heaping portion (to be fair, Chang’s does suggest diners share an order) comes spiked with chicken, shrimp, beef, and pork, not to mention an Exxon Valdez-size slick of oil. The damage? A day’s worth of calories, 1 ½ days’ worth of fat, and 2 ½ days’ worth of sodium. No meat-based dish beats out the strip.
8. Worst Appetizer
On the Border Firecracker Stuffed Jalapenos with Chili con Queso
1,950 calories – 134 g fat (36 g saturated) – 6,540 mg sodium
Appetizers are the most problematic area of most chain-restaurant menus. That’s because they’re disproportionately reliant on the type of cheesy, greasy ingredients that catch hungry diners’ eyes when they’re most vulnerable—right when they sit down. Seek out lean protein options like grilled shrimp skewers or ahi tuna when available; if not, simple is best—like chips and salsa.
9. Worst Burger
Chili’s Smokehouse Bacon Triple Cheese Big Mouth Burger with Jalapeno Ranch Dressing
1,901 calories – 138 g fat (47 g saturated) – 4,201 mg sodium
Any burger whose name is 21 syllables long is bound to spell trouble for your waistline. This burger packs almost an entire day’s worth of calories and 2 ½ days’ worth of fat. Chili’s burger menu rivals Ruby Tuesday’s for the worst in America, so you’re better off with one of their reasonable Fajita Pitas to silence your hunger.
10. Worst Sandwich
Quizno’s Large Tuna Melt
1,760 calories – 133 g fat (26 g saturated, 1.5 g trans) – 2,120 mg sodium
In almost all other forms, tuna is a nutritional superstar, so how did it end up as the headliner for America’s Worst Sandwich? Blame an absurdly heavy hand with the mayo the tuna is mixed with, along with Quiznos’ larger-than-life portion sizes. Even though they’ve managed to trim this melt down from the original 2,000-plus calorie mark when we first tested it, it still sits squarely at the bottom of the sandwich ladder.
Now you know what to avoid, and we urge you to click on the Food Matters link to read the whole list. So, if you can’t eat any of the aforementioned items what do you eat? There’s plenty to choose from. Health Life lists 100 and you can read them all by clicking on their link. Here are their top ten.
http://www.dwlz.com/HealthyLife/healthy50.html
|
THE 100 HEALTHIEST FOODS |
||
|
Fruit |
Fat/Calorie Breakdown |
Body Benefits |
|
(1) Apples |
1 medium apple: |
An apple’s 3 g of fiber help you meet your fiber goal of 20 g to 30 g daily. High-fiber diets can lower heart disease risk. |
|
(2) Apricots |
3 apricots: |
A good source of beta-carotene (which is converted to vitamin A by the body), providing the equivalent of 35% of the RDA for vitamin A |
|
(3) Bananas |
1 medium: |
Bananas are a great source of potassium, which plays a key role in heart health and muscle function. Plus each one has 2 g of fiber. |
|
(4) Blackberries |
1 cup: |
This fruit boasts a whopping 10 g of fiber in a single cup. |
|
(5) Blueberries |
1 cup: |
Blueberries help prevent and treat bladder infections by making it hard for bacteria to stick to urinary tract walls. |
|
(6) Cantaloupe |
1 cup, cubed: |
An antioxidant double whammy, with 68 mg of vitamin C and enough beta-carotene to cover 65% of your daily vitamin A quota. |
|
(7) Cherries |
1 cup: |
A good source of perillyl alcohol, which helps prevent cancer in animals. Heart-protective anthocyanins give cherries their color. |
|
(8) Cranberry |
1 cup: |
Fights bladder infections the same way blueberries do. |
|
(9) Grapefruits |
1/2 fruit: |
A good source of vitamin C and a compound called naringenin, which helps suppress tumors in animals. |
|
(10) Purple grapes |
1 cup seedless: |
Offer three heart-guarding compounds: flavonoids, anthocyanins and resveratrol. (Green grapes are not rich in them) |
If you insist on eating meat there are some good choices you can make…we’ll jump ahead on the list to give you a sneak preview.
| 74) Beef | 3 oz, cooked: 150 to 280 calories, 5 g to 20 g fat |
Beef is a good source of both CLA and iron, but since it’s also high in saturated fat, have it no more than three times a week. |
| (75) Chicken, without skin |
3 oz, cooked: 162 calories, 6 g fat |
Remove the skin and you’ve got an excellent, low fat source of protein. And 3 oz provides 38% of the RDA for the B vitamin niacin. |
| (76) Lamb | 3 oz, cooked, trimmed of fat: 175 calories, 8 g fat |
Lamb, like beef, is also a good source of CLA. Ditto beef’s saturated fat warning and weekly consumption recommendation. |
| (77) Lean pork |
3 oz, cooked, trimmed of fat: 140 calories, 4 g fat |
Fat-trimmed pork tenderloin has one-third less fat than even lean beef. And it boasts 71% of the RDA for thiamine. |
If Healthy Life doesn’t offer you enough good food ideas, here are some other excellent resources for you to peruse.
- http://tinyurl.com/lcmlalt
- http://tinyurl.com/lqg7ce8
- http://tinyurl.com/k2zzypk
- http://tinyurl.com/m9ojjbx
Bob Aronson of Bob’s Newheart is a 2007 heart transplant recipient, the founder of Facebook’s nearly 3,000 member Organ Transplant Initiative and the author of most of these donation/transplantation blogs.
You may comment in the space provided or email your thoughts to me at bob@baronson.org. And – please spread the word about the immediate need for more organ donors. There is nothing you can do that is of greater importance. If you convince one person to be an organ and tissue donor you may save or positively affect over 60 lives. Some of those lives may be people you know and love.
Please view our new music video “Dawn Anita The Gift of Life” on YouTube https://www.youtube.com/watch?v=eYFFJoHJwHs. This video is free to anyone who wants to use it and no permission is needed.
If you want to spread the word personally about organ donation, we have another PowerPoint slide show for your use free and without permission. Just go to http://www.organti.org and click on “Life Pass It On” on the left side of the screen and then just follow the directions. This is NOT a stand-alone show; it needs a presenter but is professionally produced and factually sound. If you decide to use the show I will send you a free copy of my e-book, “How to Get a Standing “O” that will help you with presentation skills. Just write to bob@baronson.org and usually you will get a copy the same day.
Also…there is more information on this blog site about other donation/transplantation issues. Additionally we would love to have you join our Facebook group, Organ Transplant Initiative The more members we get the greater our clout with decision makers.
En Espanol
Puede comentar en el espacio proporcionado o por correo electrónico sus pensamientos a mí en bob@baronson.org. Y – por favor, difundir la palabra acerca de la necesidad inmediata de más donantes de órganos. No hay nada que puedas hacer lo que es de mayor importancia. Si usted convence a una persona de ser donante de órganos y tejidos puede salvar o afectar positivamente a más de 60 vidas. Algunas de esas vidas pueden ser personas que conoces y amas.
Por favor, consulte nuestro nuevo video musical “Dawn Anita The Gift of Life” en https://www.youtube.com/watch?v=eYFFJoHJwHs YouTube. Este video es libre para cualquier persona que quiera usarlo y no se necesita permiso.
Si quieres correr la voz acerca de la donación de órganos personalmente, tenemos otra presentación de PowerPoint para su uso libre y sin permiso. Sólo tienes que ir a http://www.organti.org y haga clic en “Life Pass It On” en el lado izquierdo de la pantalla y luego sólo tienes que seguir las instrucciones. Esto no es un espectáculo independiente, sino que necesita un presentador pero es profesionalmente producida y sonido hechos. Si usted decide usar el programa le enviaré una copia gratuita de mi libro electrónico, “Cómo obtener un pie” O “que le ayudará con habilidades de presentación. Sólo tiene que escribir a bob@baronson.org y por lo general usted recibirá una copia del mismo día.
Además … hay más información sobre este sitio de blogs sobre otros donación / trasplante temas. Además nos encantaría que te unas a nuestro grupo de Facebook, la Iniciativa de Trasplante de Órganos Cuantos más miembros que obtenemos mayor será nuestra influencia con los tomadores de decisiones.
Exercise — The Simplest, Cheapest Way to Good Health
Exercise: 7 benefits of regular physical activity

You know exercise is good for you, but do you know how good? From boosting your mood to improving your sex life, find out how exercise can improve your life.
Pictures added by Bob’s NewHeart
Want to feel better, have more energy and perhaps even live longer? Look no further than exercise. The health benefits of regular exercise and physical activity are hard to ignore. And the benefits of exercise are yours for the taking, regardless of your age, sex or physical ability. Need more convincing to exercise? Check out these seven ways exercise can improve your life.
No. 1: Exercise controls weight

Exercise can help prevent excess weight gain or help maintain weight loss. When you engage in physical activity, you burn calories. The more intense the activity, the more calories you burn. You don’t need to set aside large chunks of time for exercise to reap weight-loss benefits. If you can’t do an actual workout, get more active throughout the day in simple ways — by taking the stairs instead of the elevator or revving up your household chores.
No. 2: Exercise combats health conditions and diseases

Worried about heart disease? Hoping to prevent high blood pressure? No matter what your current weight, being active boosts high-density lipoprotein (HDL), or “good,” cholesterol and decreases unhealthy triglycerides. This one-two punch keeps your blood flowing smoothly, which decreases your risk of cardiovascular diseases. In fact, regular physical activity can help you prevent or manage a wide range of health problems and concerns, including stroke, metabolic syndrome, type 2 diabetes, depression, certain types of cancer, arthritis and falls.
No. 3: Exercise improves mood

Need an emotional lift? Or need to blow off some steam after a stressful day? A workout at the gym or a brisk 30-minute walk can help. Physical activity stimulates various brain chemicals that may leave you feeling happier and more relaxed. You may also feel better about your appearance and yourself when you exercise regularly, which can boost your confidence and improve your self-esteem.
No. 4: Exercise boosts energy

Winded by grocery shopping or household chores? Regular physical activity can improve your muscle strength and boost your endurance. Exercise and physical activity deliver oxygen and nutrients to your tissues and help your cardiovascular system work more efficiently. And when your heart and lungs work more efficiently, you have more energy to go about your daily chores.
No. 5: Exercise promotes better sleep

Struggling to fall asleep? Or to stay asleep? Regular physical activity can help you fall asleep faster and deepen your sleep. Just don’t exercise too close to bedtime, or you may be too energized to fall asleep.
No. 6: Exercise puts the spark back into your sex life

Do you feel too tired or too out of shape to enjoy physical intimacy? Regular physical activity can leave you feeling energized and looking better, which may have a positive effect on your sex life. But there’s more to it than that. Regular physical activity can lead to enhanced arousal for women. And men who exercise regularly are less likely to have problems with erectile dysfunction than are men who don’t exercise.
No. 7: Exercise can be fun

Exercise and physical activity can be a fun way to spend some time. It gives you a chance to unwind, enjoy the outdoors or simply engage in activities that make you happy. Physical activity can also help you connect with family or friends in a fun social setting. So, take a dance class, hit the hiking trails or join a soccer team. Find a physical activity you enjoy, and just do it. If you get bored, try something new.
The bottom line on exercise
Exercise and physical activity are a great way to feel better, gain health benefits and have fun. As a general goal, aim for at least 30 minutes of physical activity every day. If you want to lose weight or meet specific fitness goals, you may need to exercise more. Remember to check with your doctor before starting a new exercise program, especially if you have any health concerns.
Bob Aronson of Bob’s Newheart is a 2007 heart transplant recipient, the founder of Facebook’s nearly 2,500 member Organ Transplant Initiative and the author of most of these donation/transplantation blogs.
You may comment in the space provided or email your thoughts to me at bob@baronson.org. And – please spread the word about the immediate need for more organ donors. There is nothing you can do that is of greater importance. If you convince one person to be an organ and tissue donor you may save or positively affect over 60 lives. Some of those lives may be people you know and love.
Please view our new music video “Dawn Anita The Gift of Life” on YouTube https://www.youtube.com/watch?v=eYFFJoHJwHs. This video is free to anyone who wants to use it and no permission is needed.
If you want to spread the word personally about organ donation, we have another PowerPoint slide show for your use free and without permission. Just go to http://www.organti.org and click on “Life Pass It On” on the left side of the screen and then just follow the directions. This is NOT a stand-alone show; it needs a presenter but is professionally produced and factually sound. If you decide to use the show I will send you a free copy of my e-book, “How to Get a Standing “O” that will help you with presentation skills. Just write to bob@baronson.org and usually you will get a copy the same day.
Also…there is more information on this blog site about other donation/transplantation issues. Additionally we would love to have you join our Facebook group, Organ Transplant Initiative The more members we get the greater our clout with decision makers.
En Espanol
Puede comentar en el espacio proporcionado o por correo electrónico sus pensamientos a mí en bob@baronson.org. Y – por favor, difundir la palabra acerca de la necesidad inmediata de más donantes de órganos. No hay nada que puedas hacer lo que es de mayor importancia. Si usted convence a una persona de ser donante de órganos y tejidos puede salvar o afectar positivamente a más de 60 vidas. Algunas de esas vidas pueden ser personas que conoces y amas.
Por favor, consulte nuestro nuevo video musical “Dawn Anita The Gift of Life” en https://www.youtube.com/watch?v=eYFFJoHJwHs YouTube. Este video es libre para cualquier persona que quiera usarlo y no se necesita permiso.
Si quieres correr la voz acerca de la donación de órganos personalmente, tenemos otra presentación de PowerPoint para su uso libre y sin permiso. Sólo tienes que ir a http://www.organti.org y haga clic en “Life Pass It On” en el lado izquierdo de la pantalla y luego sólo tienes que seguir las instrucciones. Esto no es un espectáculo independiente, sino que necesita un presentador pero es profesionalmente producida y sonido hechos. Si usted decide usar el programa le enviaré una copia gratuita de mi libro electrónico, “Cómo obtener un pie” O “que le ayudará con habilidades de presentación. Sólo tiene que escribir a bob@baronson.org y por lo general usted recibirá una copia del mismo día.
Además … hay más información sobre este sitio de blogs sobre otros donación / trasplante temas. Además nos encantaría que te unas a nuestro grupo de Facebook, la Iniciativa de Trasplante de Órganos Cuantos más miembros que obtenemos mayor será nuestra influencia con los tomadores de decisiones.
Mayo Clinic Preventing the Top Threats to Men’s and Women’s Health
Preventing the Top Threats to WOMEN’S Health
http://www.mayoclinic.com/health/womens-health/WO00014
At first glance one might suspect that men and women are threatened by the same health problems; cancer, heart disease, stroke and many morel And while there is some truth to that supposition there are also great differences. The Mayo Clinic, using information from the Centers for Disease Control (CDC) nicely summarized the threats and preventive steps that can and should be taken.
These tips are great reminders for everyone.
Many of the leading threats to women’s health can be prevented — if you know how. Consider this top seven list of women’s health threats, compiled from statistics provided by the Centers for Disease Control and Prevention (CDC) and other leading organizations. Then get serious about reducing your risks.
No. 1: Heart disease
Heart disease isn’t just a man’s disease — it’s also a major women’s health threat. Take charge of heart health by making healthier lifestyle choices. For example:
- Don’t smoke. If you smoke or use other tobacco products, ask your doctor to help you quit. It’s also important to avoid exposure to secondhand smoke.
- Eat a healthy diet. Choose vegetables, fruits, whole grains, high-fiber foods and lean sources of protein, such as fish. Limit foods high in saturated fat and sodium.
- Manage chronic conditions. If you have high cholesterol or high blood pressure, follow your doctor’s treatment recommendations. If you have diabetes, keep your blood sugar under control.
- Include physical activity in your daily routine. Choose sports or other activities you enjoy, from brisk walking to ballroom dancing.
- Maintain a healthy weight. Extra pounds increase the risk of heart disease.
- Limit alcohol. If you choose to drink alcohol, do so only in moderation. Too much alcohol can raise your blood pressure.
- Manage stress. If you feel constantly on edge or under assault, your lifestyle habits may suffer. Take steps to reduce stress — or learn to deal with stress in healthy ways.
No. 2: Cancer
Various types of cancer are of particular concern to women, including breast cancer, lung cancer, skin cancer and colorectal cancer. To reduce the risk of cancer, consider these general tips:
- Don’t smoke. Using any type of tobacco puts you on a collision course with cancer. Avoiding exposure to secondhand smoke counts, too.
- Maintain a healthy weight. Losing excess pounds — and keeping them off — may lower the risk of various types of cancer.
- Get moving. In addition to helping you control your weight, physical activity on its own may lower the risk of certain types of cancer.
- Eat plenty of fruits and vegetables. Although making healthy selections at the grocery store and at mealtime can’t guarantee cancer prevention, it may help reduce your risk.
- Protect yourself from the sun. When you’re outdoors, cover up and use plenty of sunscreen.
- Limit alcohol. If you choose to drink alcohol, do so only in moderation. The risk of various types of cancer — including cancer of the breast, colon, lung, kidney and liver — increases with the amount of alcohol you drink and the length of time you’ve been drinking regularly.
- Breast-feed, if you can. Breast-feeding may help reduce the risk of breast cancer.
- Take early detection seriously. Consult your doctor for regular mammograms and other cancer screenings.
No. 3: Stroke
You can’t control some stroke risk factors, such as family history, age and race. But you can control other contributing factors. For example:
- Manage chronic conditions. If you have high cholesterol or high blood pressure, follow your doctor’s treatment recommendations. If you have diabetes, keep your blood sugar under control.
- Don’t smoke. If you smoke or use other tobacco products, ask your doctor to help you quit.
- Make healthy lifestyle choices. Eat a healthy diet, being especially careful to limit foods high in saturated fat and cholesterol. Include physical activity in your daily routine. If you’re overweight, lose excess pounds.
- Limit alcohol. If you choose to drink alcohol, do so only in moderation — for women, no more than one drink a day.
No. 4: Chronic lower respiratory diseases
Chronic lung conditions — which include bronchitis and emphysema — also are a concern for women. To protect your respiratory health:
- Don’t smoke. If you smoke, ask your doctor to help you quit. Also avoid exposure to secondhand smoke.
- Steer clear of pollutants. Minimize exposure to chemicals and outdoor air pollution.
- Prevent respiratory infections. Wash your hands often and get a yearly flu vaccine. Ask your doctor whether you need a pneumonia vaccine as well.
o. 5: Alzheimer’s disease
There’s no proven way to prevent Alzheimer’s disease, but consider taking these steps:
- Manage chronic conditions. Conditions such as high blood pressure, high cholesterol, heart disease, stroke and diabetes may increase the risk of developing Alzheimer’s.
- Don’t smoke. Some research suggests a link between smoking and Alzheimer’s.
- Include physical activity in your daily routine. Any movement counts.
- Maintain social and mental fitness. Stay socially active. Practice mental exercises. Take steps to learn new things.
No. 6: Accidents
Motor vehicle crashes are a leading cause of fatal accidents among women. To stay safe on the road, use common sense. Wear your seat belt. Follow the speed limit. Don’t drive under the influence of alcohol or any other substances, and don’t drive while sleepy.
No. 7: Type 2 diabetes
Type 2 diabetes — the most common type of diabetes — affects the way your body uses blood sugar (glucose). Poorly controlled diabetes can lead to heart disease, eye problems, nerve damage and other complications. To prevent type 2 diabetes, get serious about your lifestyle choices. Eat a healthy diet. Include physical activity in your daily routine. If you’re overweight, lose excess pounds.
The bottom line
It’s important to understand common women’s health risks, but don’t feel intimidated. Instead, do whatever you can to lead a healthy lifestyle — including eating a healthy diet, staying physically active, quitting smoking and getting regular checkups. Simple preventive measures can go a long way toward reducing your health risks.
Preventing the Top Threats to MEN’S health
http://www.mayoclinic.com/health/mens-health/MC00013
The biggest threats to men’s health can often be prevented. Here’s what you need to know to live a longer, healthier life.
Do you know the greatest threats to men’s health? The list is surprisingly short — and prevention pays off. Consider this top seven list of men’s health threats, compiled from statistics provided by the Centers for Disease Control and Prevention (CDC) and other leading organizations to reflect men’s health risks in the United States. Then get serious about reducing your risks.
No. 1: Heart disease
Heart disease is a leading men’s health threat. Take charge of heart health by making healthier lifestyle choices. For example:
- Don’t smoke. If you smoke or use other tobacco products, ask your doctor to help you quit. It’s also important to avoid exposure to secondhand smoke.
- Eat a healthy diet. Choose vegetables, fruits, whole grains, high-fiber foods and lean sources of protein, such as fish. Limit foods high in saturated fat and sodium.
- Manage chronic conditions. If you have high cholesterol or high blood pressure, follow your doctor’s treatment recommendations. If you have diabetes, keep your blood sugar under control.
- Include physical activity in your daily routine. Choose sports or other activities you enjoy, from basketball to brisk walking.
- Maintain a healthy weight. Extra pounds increase the risk of heart disease.
- Limit alcohol. If you choose to drink alcohol, do so only in moderation. Too much alcohol can raise your blood pressure.
- Manage stress. If you feel constantly on edge or under assault, your lifestyle habits may suffer. Take steps to reduce stress — or learn to deal with stress in healthy ways.
No. 2: Cancer
Various types of cancer are of particular concern to men, including lung cancer, skin cancer, prostate cancer and colorectal cancer. To reduce the risk of cancer, consider these general tips:
- Don’t smoke. Using any type of tobacco puts you on a collision course with cancer. Avoiding exposure to secondhand smoke counts, too.
- Maintain a healthy weight. Losing excess pounds — and keeping them off — may lower the risk of various types of cancer.
- Get moving. In addition to helping you control your weight, physical activity on its own may lower the risk of certain types of cancer.
- Eat plenty of fruits and vegetables. Although making healthy selections at the grocery store and at mealtime can’t guarantee cancer prevention, it may help reduce your risk.
- Protect yourself from the sun. When you’re outdoors, cover up and use plenty of sunscreen.
- Limit alcohol. If you choose to drink alcohol, do so only in moderation. The risk of various types of cancer — including cancer of the colon, lung, kidney and liver — increases with the amount of alcohol you drink and the length of time you’ve been drinking regularly.
- Take early detection seriously. Consult your doctor for regular cancer screenings.
No. 3: Accidents
Motor vehicle crashes are a leading cause of fatal accidents among men. To stay safe on the road, use common sense. Wear your seat belt. Follow the speed limit. Don’t drive under the influence of alcohol or any other substances, and don’t drive while sleepy.
No. 4: Chronic lower respiratory diseases
Chronic lung conditions — which include bronchitis and emphysema — also are a concern for men. To protect your respiratory health:
- Don’t smoke. If you smoke, ask your doctor to help you quit. Also avoid exposure to secondhand smoke.
- Steer clear of pollutants. Minimize exposure to chemicals and outdoor air pollution.
- Prevent respiratory infections. Wash your hands often and get a yearly flu vaccine. Ask your doctor whether you need a pneumonia vaccine as well.
No. 5: Stroke
You can’t control some stroke risk factors — such as family history, age and race — but you can control other contributing factors. For example:
- Manage chronic conditions. If you have high cholesterol or high blood pressure, follow your doctor’s treatment recommendations. If you have diabetes, keep your blood sugar under control.
- Don’t smoke. If you smoke or use other tobacco products, ask your doctor to help you quit.
- Make healthy lifestyle choices. Eat a healthy diet, being especially careful to limit foods high in saturated fat and cholesterol. Include physical activity in your daily routine. If you’re overweight, lose excess pounds.
- Limit alcohol. If you choose to drink alcohol, do so only in moderation.
No. 6: Type 2 diabetes
Type 2 diabetes — the most common type of diabetes — affects the way your body uses blood sugar (glucose). Poorly controlled diabetes can lead to heart disease, eye problems, nerve damage and other complications. To prevent type 2 diabetes, get serious about your lifestyle choices. Eat a healthy diet. Include physical activity in your daily routine. If you’re overweight, lose excess pounds.
No. 7: Suicide
Suicide is another leading men’s health risk. An important risk factor for suicide among men is depression. If you have signs and symptoms of depression — such as feelings of sadness or unhappiness and loss of interest in normal activities — consult your doctor. Treatment is available. If you’re contemplating suicide, call for emergency medical help or go the nearest emergency room.
The bottom line
Understanding health risks is one thing. Taking action to reduce your risks is another. Start with healthy lifestyle choices — eating a healthy diet, staying physically active, quitting smoking, getting regular checkups and taking precautions in your daily activities. The impact may be greater than you’ll ever know.
Bob Aronson of Bob’s Newheart is a 2007 heart transplant recipient, the founder of Facebook’s nearly 2,500 member Organ Transplant Initiative and the author of most of these donation/transplantation blogs.
You may comment in the space provided or email your thoughts to me at bob@baronson.org. And – please spread the word about the immediate need for more organ donors. There is nothing you can do that is of greater importance. If you convince one person to be an organ and tissue donor you may save or positively affect over 60 lives. Some of those lives may be people you know and love.
Please view our video “Thank You From the Bottom of my Donor’s heart” on http://www.organti.org This video was produced to promote organ donation so it is free and no permission is needed for its use.
If you want to spread the word personally about organ donation, we have another PowerPoint slide show for your use free and without permission. Just go to http://www.organti.org and click on “Life Pass It On” on the left side of the screen and then just follow the directions. This is NOT a stand-alone show; it needs a presenter but is professionally produced and factually sound. If you decide to use the show I will send you a free copy of my e-book, “How to Get a Standing “O” that will help you with presentation skills. Just write to bob@baronson.org and usually you will get a copy the same day.
Also…there is more information on this blog site about other donation/transplantation issues. Additionally we would love to have you join our Facebook group, Organ Transplant Initiative The more members we get the greater our clout with decision makers.
Espanol
Bob Aronson Newheart de Bob es un receptor de trasplante cardiaco 2007, el fundador de Facebook, casi 2.500 Iniciativa miembro de Trasplante de Órganos y el autor de la mayoría de los blogs de donación / trasplante.
Puede comentar en el espacio proporcionado o por correo electrónico sus pensamientos a mí en bob@baronson.org. Y – por favor, difundir la palabra acerca de la necesidad inmediata de más donantes de órganos. No hay nada que puedas hacer lo que es de mayor importancia. Si usted convence a una persona de ser donante de órganos y tejidos puede salvar o afectar positivamente a más de 60 vidas. Algunas de esas vidas pueden ser personas que conoces y amas.
Por favor vea nuestro video “Gracias desde el fondo de mi corazón Donante” en http://www.organti.org Este video fue producido para promover la donación de órganos por lo que es libre y no se necesita permiso para su uso.
Si quieres correr la voz acerca de la donación de órganos personalmente, tenemos otra presentación de PowerPoint para su uso libre y sin permiso. Sólo tienes que ir a http://www.organti.org y haga clic en “Life Pass It On” en el lado izquierdo de la pantalla y luego sólo tienes que seguir las instrucciones. Esto no es un espectáculo independiente, sino que necesita un presentador pero es profesionalmente producida y sonido hechos. Si usted decide usar el programa le enviaré una copia gratuita de mi libro electrónico, “Cómo obtener un pie” O “que le ayudará con habilidades de presentación. Sólo tiene que escribir a bob@baronson.org y por lo general usted recibirá una copia del mismo día.
Además … hay más información sobre este sitio de blogs sobre otros donación / trasplante temas. Además nos encantaría que te unas a nuestro grupo de Facebook, la Iniciativa de Trasplante de Órganos Cuantos más miembros que obtenemos mayor será nuestra influencia con los tomadores de decisiones.

You must be logged in to post a comment.